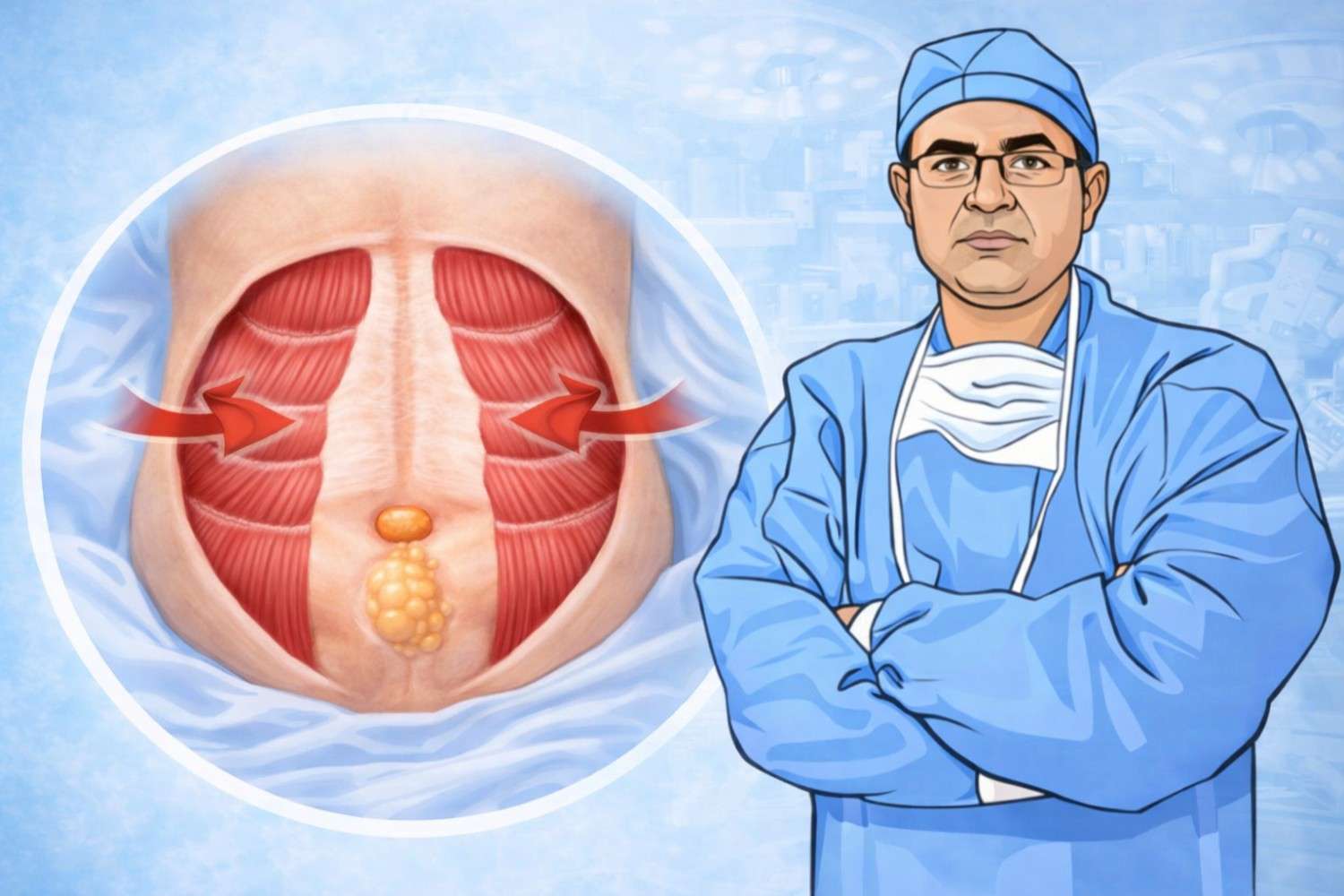
Understanding Divarication of Recti
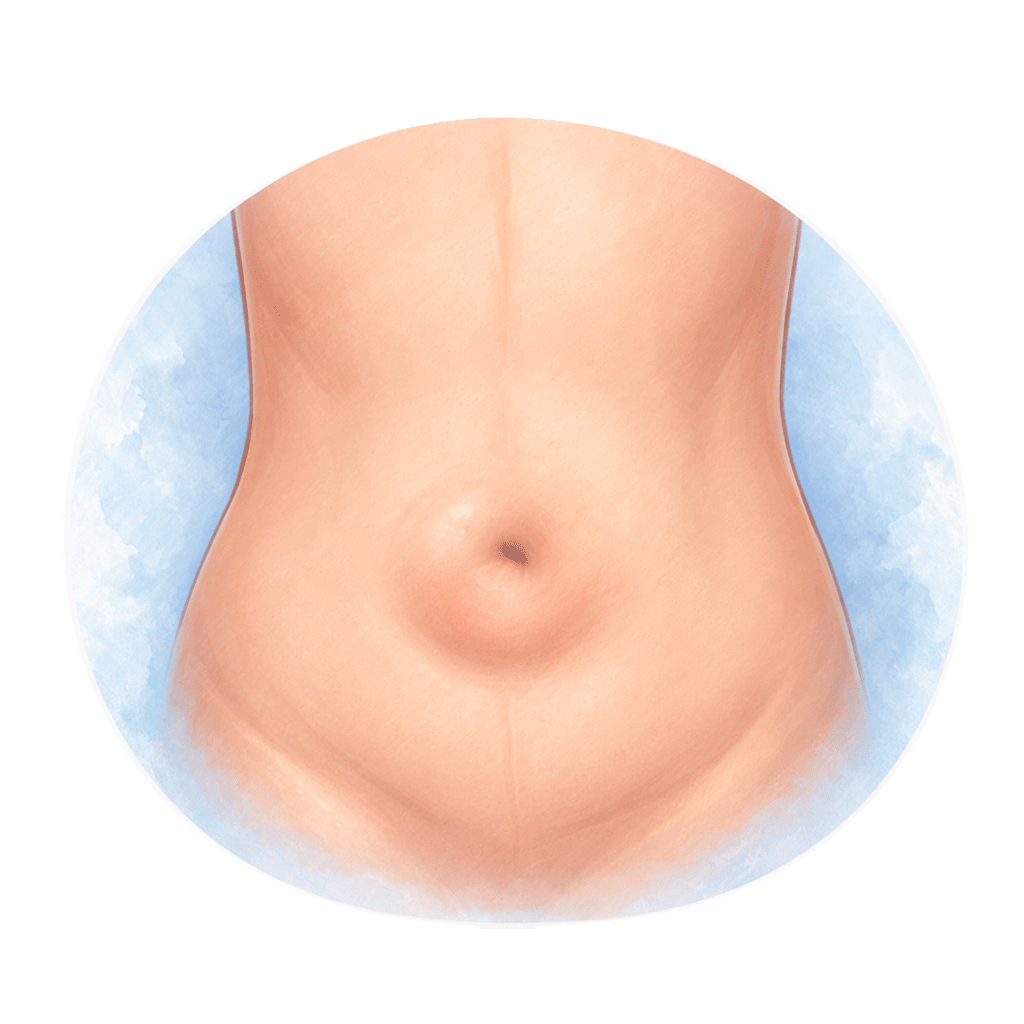
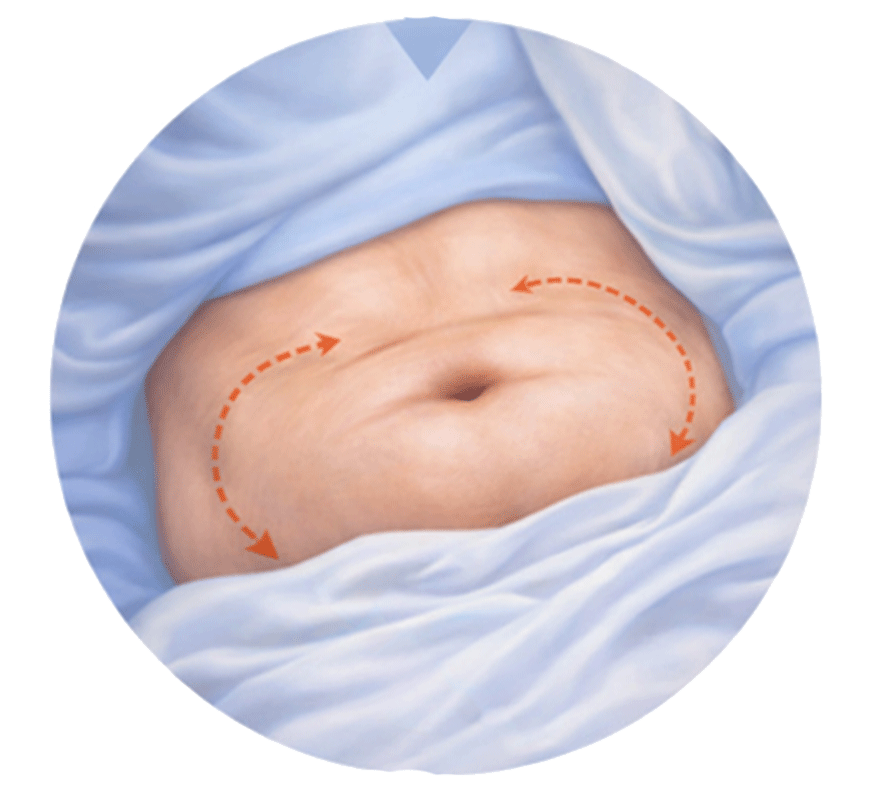
The rectus abdominis muscles run vertically on either side of the abdomen and help maintain core strength and posture. When the connective tissue between them becomes stretched or weakened, the muscles move apart, creating a midline bulge.
Unlike a hernia, divarication of recti does not involve a defect in the abdominal wall. However, it may coexist with umbilical or ventral hernias in some individuals.