Colorectal Surgery
Expertise. Precision. Compassion.
Advanced surgical care for conditions of the colon, rectum, and anus — by a fellowship-trained specialist with international standards of practice.
Dr. Rajeev Kapoor
Additional Director — Oncology & Colorectal Surgery, Fortis Hospital Mohali
Dr. Rajeev Kapoor is a fellowship-trained specialist in colorectal surgery with double board-certification and an accredited fellowship from Australia. Over 35 years of practice, he has performed more than 20,000 surgical procedures — bringing international standards of care to patients across Chandigarh, Mohali, Panchkula, and Punjab.
His clinical scope spans the full colorectal spectrum — from colon cancer and rectal cancer to piles, fistula, and inflammatory bowel disease — alongside hernia, gallbladder, and emergency surgical care at Fortis Hospital Mohali.

Dr. Kapoor provides specialist surgical care across the full range of colorectal, anal, and cancer conditions. Click on any condition to learn more.
The colon and rectum — 3D anatomical illustration
Colorectal Cancer
Comprehensive surgical management of colon cancer and rectal cancer — including laparoscopic, robotic, and sphincter-preserving surgeries. Multidisciplinary care with oncology, radiology, and pathology.
Colorectal cancer is one of the most common cancers globally, yet outcomes are significantly better when detected at an early stage — underscoring the importance of timely screening.
Inflammatory Bowel Disease (IBD)
Surgical and non-surgical management of Crohn's disease and Ulcerative Colitis. When surgery is needed, minimally invasive procedures are used to preserve as much bowel function as possible.
IBD affects millions globally and is increasingly common in India. Surgery is considered when medical management is insufficient or when complications such as strictures or fistulas develop.
Diverticular Disease
Surgical care for complications of diverticulitis — including strictures, fistulas, and perforations — using bowel-preserving techniques tailored to the individual patient.
Diverticula are small pouches that can form in the colon wall, most commonly after age 50. In a proportion of cases, these become inflamed (diverticulitis) and may require surgical intervention.
Anorectal Disorders
Surgical management options for piles (hemorrhoids), anal fistula, anal fissures, and pilonidal sinus. Laser proctology and minimally invasive techniques are among the options evaluated for each patient.
Haemorrhoids are among the most prevalent anorectal conditions, affecting a large proportion of adults. Most cases are managed conservatively; surgery is recommended for advanced or recurrent presentations.
Rectal Prolapse
Surgical correction of prolapsed rectum using laparoscopic and robotic techniques aimed at restoring bowel function and reducing symptoms.
Rectal prolapse occurs when the rectum loses its internal attachments and slides outside the body. It is more common in women and older adults, and is a surgically correctable condition.
Colostomy & Stoma Care
Creation and management of stomas — including colostomy and ileostomy. Certified stoma therapists provide pre- and post-operative education, rehabilitation guidance, and ongoing support.
A stoma is a surgically created opening that allows waste to exit the body when normal bowel function is not possible. With appropriate support and education, most patients adapt well to life with a stoma.
Colorectal Polyps
Detection and removal of colorectal polyps before they develop into cancer. Regular colonoscopy is the gold standard for early detection.
Most colorectal cancers develop from polyps over a period of years — making colonoscopy one of the most effective available tools for cancer prevention through early detection and removal.
Other Conditions
Also treated: fecal incontinence, perianal abscess, radiation proctitis, anal incontinence, appendiceal cancer, and colonic obstruction.
Fecal incontinence is significantly under-reported due to social stigma, yet it is a treatable condition. Patients are encouraged to seek assessment — effective surgical and non-surgical management options exist.
The right surgical approach is chosen based on your specific condition, overall health, and what will give you the best outcome. Dr. Kapoor is skilled in all three approaches.
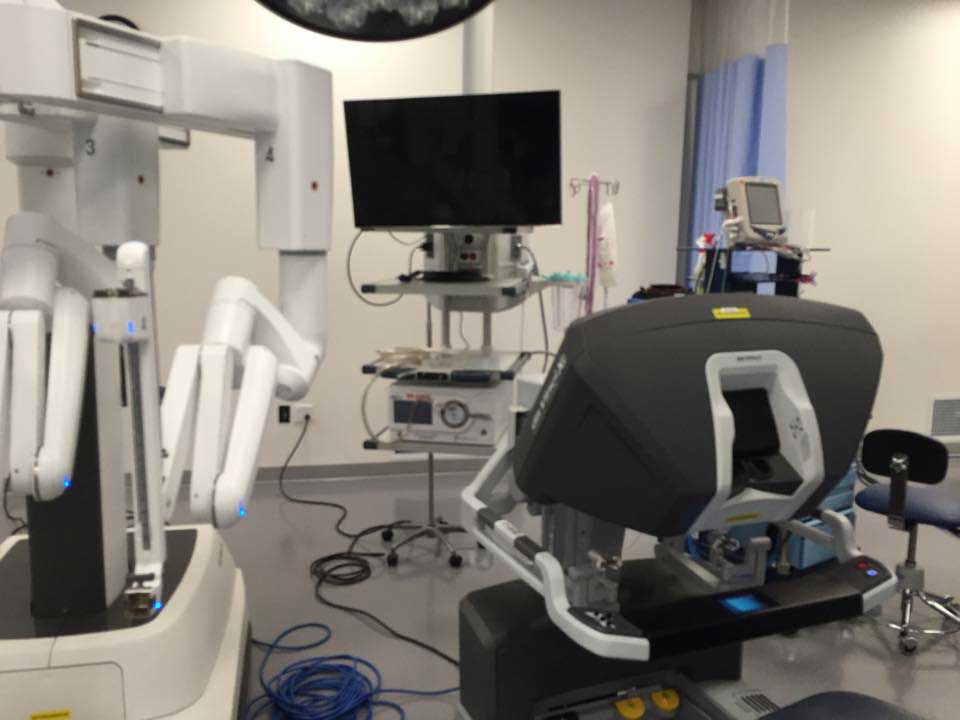
Robotic Surgery
The da Vinci robotic system gives the surgeon exceptional precision and three-dimensional vision inside the pelvis — especially valuable for rectal cancer and complex pelvic conditions. Minimally invasive approach, with smaller incisions for many patients.
Learn about robotic surgery →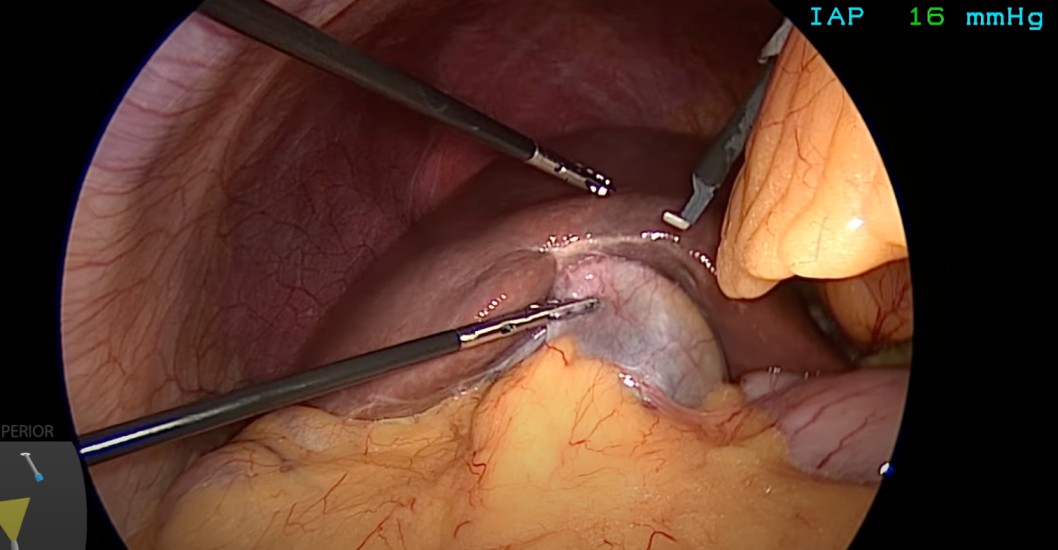
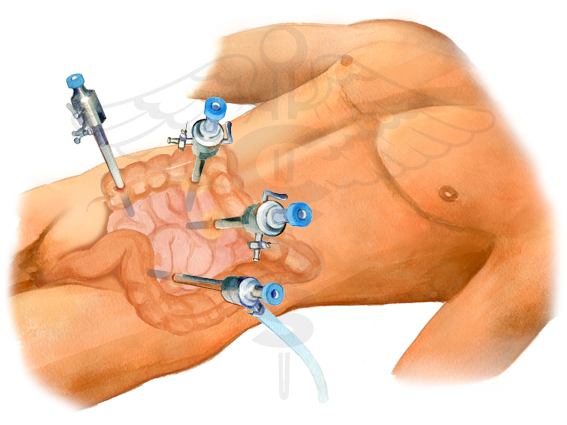
Laparoscopic (Keyhole) Surgery
Most colorectal procedures can be done through tiny incisions using a camera and fine instruments. Many patients experience shorter hospital stays and a graduated return to daily activities, depending on individual circumstances.
Learn about laparoscopic surgery →
Open Surgery
Some complex cancers or emergency situations require an open approach for the safest outcome. This is not inferior — in the right hands, open surgery achieves excellent results with careful, experienced technique.
Learn about open surgery →
Annotated CT scan — used in planning colorectal surgery
Knowledge helps patients make better decisions. The Patient Learning Centre has plain-language guides on everything from preparing for your colonoscopy to recovering after surgery.

Colonoscopy — the gold standard test for detecting colorectal cancer early
While Dr. Kapoor's specialist focus is colorectal and cancer surgery, his surgical training and clinical practice cover the full breadth of general and emergency surgery. Patients across Chandigarh, Mohali, and Panchkula seek his care for a wide range of abdominal conditions.
Hernia Surgery
Repair of inguinal, umbilical, incisional, and hiatus hernias — using laparoscopic (keyhole) and open techniques. Mesh repair and tension-free procedures using established surgical techniques guided by each patient's clinical profile.
Hernia surgery →Gallbladder Surgery
Laparoscopic cholecystectomy (gallbladder removal) for gallstones, cholecystitis, and biliary conditions. Day-care or short-stay procedures, with return to activity at a pace guided by the surgical team.
Gallbladder surgery →Emergency Surgery
Round-the-clock emergency surgical care for acute abdominal crises — bowel obstruction, perforations, peritonitis, and acute appendicitis. Dr. Kapoor and the Fortis team are available when surgery cannot wait.
Emergency surgery →General Abdominal Surgery
Appendectomy, splenectomy, small bowel surgery, abdominal wall reconstruction, and a full range of general surgical procedures — delivered with the same precision and care as his specialist colorectal work.
All surgical services →For a complete list of conditions and procedures, visit the Services page or contact the clinic directly.
Contact Information
Dr. Rajeev Kapoor — Additional Director, Oncology & Colorectal Surgery
📍 Fortis Hospital, Sector 62, Phase 8, Mohali, Punjab — 160062
📞 +91 98765 07444 |
✉️ rkap01@gmail.com
For appointments or enquiries: Contact page | drrajeevkapoor.com