Fecal Incontinence — Surgery Can Set You Free
Years of staining clothes, running to the washroom, or living with a stoma need not be your future. Surgery has restored bowel control — and dignity — for patients from across India and neighbouring countries.
“Treating fecal incontinence by surgery is my forte. I perform overlapping sphincteroplasty and pelvic floor reconstruction — and have helped patients from across India and neighbouring countries regain their bowel control and their quality of life.”
— Dr. Rajeev Kapoor, Colorectal & Cancer SurgeonWhat You Need to Know
- Fecal incontinence is common and treatable — it affects millions of adults and can be significantly improved with the right care.
- There are two main types: urge incontinence (you feel a sudden urge but can't reach the toilet in time) and passive incontinence (stool leaks without any warning or sensation).
- The most common cause in women is sphincter damage during childbirth — symptoms can appear immediately or decades later.
- Surgery works — overlapping sphincteroplasty and sacral nerve stimulation restore bowel control in the majority of patients. Conservative measures are tried first, but surgery delivers the best long-term results when the sphincter is damaged.
- You should not have to live with this condition. Most people can be meaningfully helped. A specialist assessment is the first step.
What Is Fecal Incontinence?
Fecal incontinence (also called anal incontinence) is the inability to control when you pass stool. Stool leaks before you can reach a toilet — or sometimes without any warning at all.
It can range from occasionally leaking a small amount of stool when passing wind, to a complete and sudden loss of bowel control. It may involve liquid stool, solid stool, or just mucus.
Many people are embarrassed to tell their doctor about this problem — but it is far more common than most people realise, and it is treatable. You do not have to suffer in silence.
How common is it? Studies suggest fecal incontinence affects 2–15% of adults worldwide. In India, estimates range from 1–3% of the general population — though the true number is likely higher because many people never report it. It is more common in women and increases with age.

What Causes Fecal Incontinence?
The most common cause is a tear or weakening of the anal sphincter — the ring of muscle that keeps your bowel closed. This can happen for several reasons.
Childbirth Injury
The most common cause in women. Prolonged labour, forceps delivery, a large tear, or an infected episiotomy scar can damage the anal sphincter. Symptoms sometimes appear years after delivery.
Previous Anal Surgery
Operations for haemorrhoids, anal fistula, or anal fissure can occasionally damage sphincter muscle or the nerves controlling it, leading to incontinence.
Nerve Damage
Diabetes, multiple sclerosis, spinal injury, or years of chronic straining can damage the pudendal nerves — the nerves that tell the sphincter when to contract and relax.
Rectal Prolapse
When the rectum slides out of its normal position, it stretches the sphincter over time and disrupts the normal signals that maintain continence.
IBD & Diarrhoea
Inflammatory bowel disease (Crohn's disease, ulcerative colitis) causes urgency and loose stools that are difficult to hold, especially if the sphincter is already weakened.
Ageing
The sphincter muscle naturally weakens with age. Older adults may find that previously manageable urgency becomes harder to control. This is treatable — it is not something to accept.
Symptoms & How It Affects Life
Fecal incontinence can present in different ways. You might experience one or several of these symptoms.
- An urgent need to use the toilet with very little time to reach it
- Leakage of liquid or formed stool without warning
- Soiling underclothes, especially when passing wind
- Passing stool during sleep
- Passing mucus without any stool
- Skin irritation, itching, or soreness around the anus
⚡ Urge Incontinence
You feel a sudden, powerful urge to open your bowel and cannot hold it long enough to reach a toilet. There is some warning, but not enough. Often linked to poor sphincter squeeze pressure or rectal hypersensitivity.
💧 Passive Incontinence
Stool leaks without any sensation or warning — you may be unaware it is happening until you notice it. Usually caused by damage to the internal anal sphincter or impaired nerve signalling. Common after anal surgery or radiation.
Please don’t delay: Many patients spend years — sometimes decades — managing this condition alone, avoiding social situations, and declining in quality of life. There is effective treatment available. The sooner you seek help, the better the results.

Emotional impact: Fecal incontinence causes deep embarrassment, anxiety, and social isolation. It affects marriages, friendships, and careers. Recognising this emotional toll is part of good medical care.
How Is It Diagnosed?
A thorough evaluation helps identify the underlying cause and guides the right treatment. Dr. Kapoor will take a detailed history and examine you before recommending tests.
History & Clinical Examination
A detailed discussion of your symptoms, obstetric history, previous surgeries, bowel habits, and medications. The clinical examination is critical — a careful examination of the anal canal gives very clear information about the integrity and function of the sphincter. By mapping the deficit in the muscle during the examination, it is possible in most cases to precisely identify whether a gap in the sphincter muscle exists and where it lies. This is one of the most important steps in the entire assessment — and an experienced colorectal surgeon will draw significant diagnostic information from it before any investigation is requested.
Anorectal Manometry
A small probe placed in the anal canal measures the pressure your sphincter generates at rest and when you squeeze. This tells us how strong your sphincter muscles are and whether nerve function is intact.
Endoanal Ultrasound
A small ultrasound probe is placed in the anal canal to produce detailed images of the sphincter. This identifies tears, thinning, or scarring in the muscle — which is the most important factor in deciding whether surgery will help.
MRI of the Pelvis & Sphincter
MRI provides detailed images of the sphincter anatomy and surrounding pelvic floor. It tells us the precise anatomy of any defect in the sphincter muscle and — crucially — the completeness of that defect. This distinction matters greatly: partial sphincter defects can often be managed with pelvic floor exercises and conservative measures, whereas complete defects are best treated surgically with sphincter repair. MRI is an important investigation before planning any sphincteroplasty.
Pudendal Nerve Latency Test (selected cases)
Measures how quickly signals travel along the nerves that control the sphincter. Significant nerve damage may affect the choice of treatment and predicted outcomes from surgery.
Balloon Expulsion Test
A small water-filled balloon is placed in the rectum and you are asked to expel it while sitting on a commode. If you are unable to expel it within the normal time range, it suggests a problem with rectal emptying or pelvic floor coordination (dyssynergia) — which changes the treatment plan significantly.
Electromyography / EMG (specialist centres)
Electromyography maps the electrical activity of the sphincter muscles and their nerve supply. It can identify precise areas of denervation (nerve-damaged muscle) that are not visible on ultrasound. Used in complex cases where the degree of nerve damage needs to be accurately mapped before deciding on surgery.

Non-Surgical Treatment
Most patients start with conservative measures. For many, these alone can provide significant relief — especially when incontinence is mild to moderate.
| Treatment | What It Involves | Best For |
|---|---|---|
| Dietary changes | High-fibre diet, regular meal times, adequate fluid intake. Avoiding trigger foods (spicy food, caffeine, fatty meals, excess dairy). | Loose stools and urgency; as a first step for all patients |
| Bowel management | Scheduled toileting at predictable times each day to reduce unpredictable accidents. Avoiding straining. | All patients; especially those with constipation or unpredictable timing |
| Pelvic floor exercises | Kegel exercises to strengthen the sphincter and pelvic floor muscles. Done correctly, these significantly improve squeeze pressure. | Mild to moderate incontinence; post-delivery recovery |
| Biofeedback therapy | Sensors monitor muscle activity and provide real-time feedback so you learn to contract the right muscles at the right time. Typically 6–8 sessions. | Patients with functioning muscles but poor coordination or awareness |
| Medications | Loperamide (slows gut movement and firms stool), stool bulking agents (psyllium husk, ispaghula). Used to optimise stool consistency. | Loose or liquid stools; diarrhoea-predominant incontinence |
| Transanal irrigation | A device introduces water into the rectum to empty it at a predictable time, reducing unexpected accidents for the rest of the day. | Patients with incomplete emptying or neurogenic bowel |
Surgical Treatment Options
When conservative measures have not provided enough relief, several surgical options are available. The right choice depends on the cause, the degree of sphincter damage, and individual circumstances.
Sphincteroplasty (Overlapping Sphincter Repair)
The standard operation for incontinence caused by a tear in the anal sphincter — most commonly from childbirth injury. The torn ends of the muscle are identified, mobilised, and overlapped over each other, then stitched together to reconstruct the muscle ring. Recovery takes 4–6 weeks. About 60–80% of carefully selected patients achieve a significant improvement in bowel control.
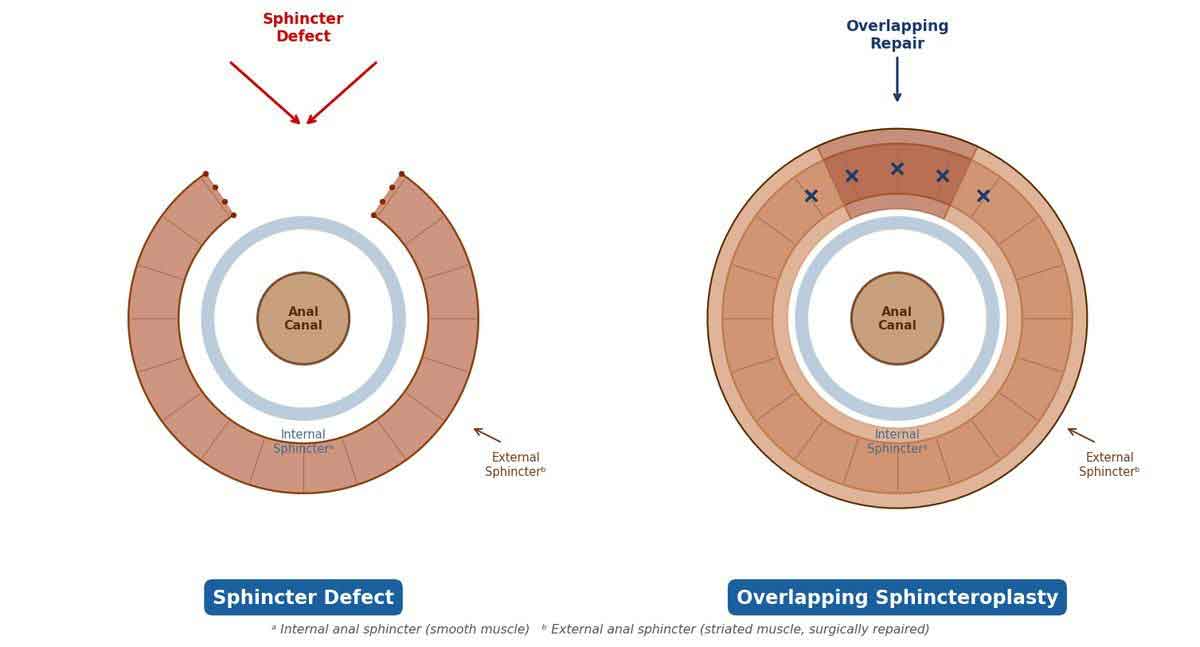
Left: Sphincter defect — gap in the muscle ring | Right: Overlapping sphincteroplasty — muscle ends overlapped and sutured
Sacral Nerve Stimulation (SNS / InterStim™)
A small pulse generator is implanted near the lower spine (sacrum) and delivers gentle, continuous electrical impulses to the sacral nerves that control bowel function. It works by improving the communication between the brain, nerves, and sphincter muscles. It is especially effective when the sphincter is intact but poorly coordinated, or when there is only mild muscle damage. A trial period is done first to confirm benefit before permanent implantation. About 60–80% of patients experience meaningful improvement.
Injection of Bulking Agents
A bulking material (such as silicone microspheres) is injected into the tissue just inside the anal canal. This narrows the anal opening slightly, improving the seal. It is a minor, quick procedure, usually done under local anaesthesia. Best suited to mild incontinence, particularly passive leakage (leakage without urgency). Results vary — it is not a permanent solution but can provide months to years of improvement with minimal downtime.
Antegrade Continence Enema (ACE / Malone Procedure)
The ACE procedure creates a small channel (usually using the appendix or a section of bowel) between the skin of the abdomen and the colon. This allows you to flush the bowel with a warm saline solution at a predictable time each day, keeping the colon empty and preventing accidents. It is particularly helpful for patients with neurogenic bowel (due to spinal injury, multiple sclerosis, or congenital conditions) and for those with mixed incontinence and constipation. Recovery is straightforward; most patients achieve a high degree of independence.
Dynamic Graciloplasty
The gracilis muscle (from the inner thigh) is wrapped around the anal canal to create a new sphincter. An implanted electrical stimulator keeps the muscle in a sustained contraction, maintaining continence. You press a magnet near the device to relax it when you want to open your bowel. A major operation, reserved for patients with severe incontinence when other surgical options have failed or are not suitable. Performed in specialist centres only.
Artificial Bowel Sphincter
An inflatable silicone cuff is placed around the anal canal and connected to a pressure-regulating balloon and a small pump placed in the scrotum or labia. Squeezing the pump deflates the cuff to allow a bowel movement; the cuff reinflates automatically. Effective but has a recognised risk of device infection and mechanical failure requiring reoperation. Reserved for selected patients with severe incontinence and no suitable alternative.
Colostomy (Stoma Surgery)
When all other treatments have failed, or when the sphincter is irreparably damaged, a colostomy creates an opening in the abdomen through which the bowel empties into a bag worn on the skin. While this sounds drastic, many patients who have lived for years with uncontrolled leakage describe the colostomy as a life-changing improvement — giving them freedom to travel, socialise, and work without fear. It is a carefully considered, last-resort option — not a failure.
Which surgery is right for you? This depends entirely on your examination findings, the results of your anorectal manometry and endoanal ultrasound, and how much your symptoms affect your daily life. Dr. Kapoor will discuss all the options, their likely outcomes, and what to expect from each — so you can make an informed decision.
Frequently Asked Questions
While some very mild leakage in the early weeks after delivery can occur as the pelvic floor recovers, persistent fecal incontinence is not normal. It usually means the anal sphincter was torn during delivery. This is a treatable condition — do not assume you have to live with it. Many women suffer for years unnecessarily before seeking help.
Pelvic floor exercises can significantly improve mild to moderate fecal incontinence, especially when the sphincter muscle is intact but weak. When combined with biofeedback therapy, results are often better. For incontinence caused by a sphincter tear, exercises alone are usually not sufficient and a surgical repair gives better outcomes.
Sphincteroplasty (overlapping sphincter repair) is an operation to repair a damaged or torn anal sphincter by overlapping and stitching the muscle ends together. It is the standard surgical treatment for incontinence caused by childbirth injury. About 60–80% of patients achieve a significant improvement in bowel control. Long-term results are best when surgery is done before the nerve supply to the muscle deteriorates.
Sacral nerve stimulation (SNS) is a procedure where a small pulse generator is implanted near the lower spine and sends gentle impulses to the sacral nerves that control bowel function. It works well for patients with a functioning sphincter that is not contracting properly, or with mild sphincter damage. It is less useful when there is a large structural tear that needs direct repair. About 60–80% of carefully selected patients experience significant improvement.
A colostomy is only considered when all other treatments have been tried and have not helped, or when the sphincter is so severely damaged that repair is not possible. The vast majority of patients can be managed with non-surgical treatment, biofeedback, sphincteroplasty, or sacral nerve stimulation without needing a stoma. A colostomy is a carefully considered last resort — not a routine outcome for fecal incontinence.
No. While the sphincter does weaken slightly with age, significant fecal incontinence is a medical condition that should be evaluated and treated. Many older patients respond very well to conservative treatment or minimally invasive procedures. Age alone should not stop you from seeking help — quality of life matters at every age.
Most patients are in hospital for 2–3 days after overlapping sphincteroplasty. Full recovery takes approximately 4–6 weeks, during which strenuous activity and heavy lifting are avoided. Bowel function gradually improves over 3–6 months as the repaired muscle strengthens. Most patients can return to desk work within 2–3 weeks.
Yes — the vast majority of patients are treated successfully without a stoma. Depending on the cause and severity, treatment options include pelvic floor physiotherapy, biofeedback, dietary changes, overlapping sphincteroplasty (sphincter repair), or sacral nerve stimulation. A colostomy is only considered as a last resort when all other options have been exhausted or the sphincter is irreparably damaged.
Living with Fecal Incontinence
While you wait for or recover from treatment, practical strategies can help you manage day-to-day life and protect your skin and confidence.
Skin Protection
Clean the skin around the anus gently with water after each episode — avoid harsh soaps. Apply a barrier cream (zinc oxide or petroleum jelly) to protect against moisture and irritation. Use soft, unscented wipes rather than rubbing.
Food & Drink
Keep a food diary to identify triggers. Common culprits include spicy food, caffeine, alcohol, fatty meals, and excess dairy. Eating at regular times and avoiding large meals before outings can reduce urgency.
Going Out
Plan toilet access before leaving home. Apps such as the Great British Toilet Map (usable globally) or Toilet Finder help locate public facilities. Carrying a small hygiene kit and a change of underwear can reduce anxiety significantly.
Night-time
Use a waterproof mattress protector. Avoid heavy meals within two hours of bedtime. Some patients find that a light snack rather than a full dinner reduces night-time episodes. Discuss timing of medications with your doctor.
Exercise & Activity
Do not stop exercising — physical activity supports bowel regularity and overall health. Time exercise after your predictable morning bowel routine. Avoid high-impact activities immediately after eating. Swimming and walking are especially manageable.
Emotional Support
Fecal incontinence is a medical condition, not a personal failing. Many patients find it helpful to speak with a counsellor or join a support group. Sharing your situation with a trusted partner or family member can relieve the burden of secrecy.
⚠️ When to Contact Your Doctor Urgently
- Sudden and complete loss of bowel control that was not present before
- Blood in the stool or significant rectal bleeding
- New incontinence after recent pelvic or colorectal surgery
- Incontinence accompanied by new lower back pain or leg weakness (may indicate nerve compression)
- Significant unexplained weight loss alongside bowel symptoms
- Skin around the anus that is severely broken, infected, or not healing
Key Points — Fecal Incontinence
- Fecal incontinence has two forms: urge (sudden warning) and passive (no warning) — they have different causes and different treatments.
- A careful clinical examination and MRI of the perineum are the cornerstones of diagnosis — together they define the exact extent of the sphincter defect and determine whether surgery will help.
- Sphincteroplasty (overlapping sphincter repair) and sacral nerve stimulation (SNS) are the two most effective surgical options for the majority of patients.
- Conservative treatment — diet, pelvic floor exercises, and biofeedback — should be tried first and continues alongside any surgical treatment.
- Colostomy is a last resort, not a routine outcome. The vast majority of patients can be managed without a stoma.
- The sooner you seek help, the better the results — nerve damage to the sphincter accumulates over time and reduces surgical success rates.
Sphincter Reconstruction & Pelvic Floor Surgery
Overlapping sphincteroplasty — the surgical repair of the anal sphincter — and pelvic floor reconstruction are among Dr. Kapoor's primary surgical specialities. He has assessed and treated patients with fecal incontinence from across India and from neighbouring countries.
If you or someone you know has been living with incontinence, a specialist assessment can identify the underlying cause and outline the most appropriate treatment.
Request a Consultation →

For appointments or enquiries: Contact page | drrajeevkapoor.com