Colonoscopy in Chandigarh & Mohali
A complete guide to colonoscopy — what it is, how to prepare, what happens during the procedure, and what to expect afterwards.
What Is a Colonoscopy?
A colonoscopy is a procedure in which a thin, flexible tube with a tiny camera at its tip — called a colonoscope — is gently passed through the anus into the large bowel (colon and rectum). It allows the surgeon to view the inner lining of the entire large intestine on a monitor, look for abnormalities, and, in many cases, treat them at the same time.
The colonoscope is about 1.5 metres long and roughly as thick as an adult finger. It carries its own light source and a small channel through which instruments can be passed — for taking biopsies, removing polyps, or controlling bleeding.
Colonoscopy is currently the most accurate test available for examining the large bowel. It provides a direct, real-time view of the bowel lining and allows treatment to be performed at the same time — something no other bowel-imaging test can do.
Dr. Kapoor holds formal accreditation in diagnostic and therapeutic colonoscopy from the Gastroenterological Society of Australia (GESA) — one of the most rigorous colonoscopy credentialling bodies in the world — awarded in 2001. This accreditation confirms competency in both diagnostic examination and therapeutic interventions such as polypectomy performed during colonoscopy.
Important: Colonoscopy requires a clean (empty) bowel. This is why preparation — called bowel prep — is done the day before. Good bowel preparation is the single most important factor in the quality and accuracy of a colonoscopy. See full preparation guide ↓

The large bowel is approximately 1.5 metres long and consists of the cecum, ascending colon (right side), transverse colon (across the top of the abdomen), descending colon (left side), sigmoid colon (S-shaped loop in the pelvis), rectum, and anus. The colonoscope travels through all of these sections from the anus to the cecum — and, if possible, into the last part of the small bowel (terminal ileum).

Key landmarks the doctor looks for:
- Ileocaecal valve — confirms the scope has reached the beginning of the large bowel; important quality marker
- Appendix orifice — the opening of the appendix, visible inside the cecum
- Hepatic and splenic flexures — bends where the colon turns; technically challenging areas that require skill to navigate
- Rectosigmoid junction — a tight S-shaped bend that is examined carefully on the way out
Most cancers and pre-cancerous polyps in the large bowel develop in the left colon and rectum — the areas examined last on insertion and first on withdrawal. The withdrawal phase of the procedure (pulling the scope back slowly) is when most abnormalities are detected, and a minimum withdrawal time of 6 minutes is recommended as a quality standard.
Why Is a Colonoscopy Recommended?
A colonoscopy may be recommended for diagnostic reasons (investigating a symptom) or as a routine screening test. The most common reasons include:
Rectal Bleeding or Blood in the Stool
Bright red or dark blood in the stools, blood mixed with stool, or blood noticed on toilet paper should always be investigated. While haemorrhoids are the most common cause, a colonoscopy is often needed to rule out polyps, colitis, or cancer.
Change in Bowel Habits
A persistent change lasting more than 3–4 weeks — such as looser stools, increased frequency, constipation, or alternating patterns — that cannot be explained by diet or medication warrants investigation.
Colorectal Cancer Screening
Colonoscopy is the gold-standard screening test for bowel cancer. Routine screening is recommended from age 45 for average-risk individuals, and earlier for those with a family history of colorectal cancer or polyps. Learn about screening guidelines.
Polyp Surveillance
If you have had polyps removed in the past, colonoscopy at regular intervals (surveillance) is needed to check for new polyps before they can develop into cancer. The interval depends on the type and number of polyps previously found.
Inflammatory Bowel Disease (IBD)
Colonoscopy is used to diagnose and monitor Crohn's disease and ulcerative colitis, assess the extent and severity of inflammation, take biopsies, and check for dysplasia (early cellular changes) in patients with long-standing colitis.
Unexplained Anaemia or Abdominal Pain
Iron-deficiency anaemia without an obvious cause, or persistent abdominal pain, can be signs of a bleeding lesion or tumour in the bowel. Colonoscopy is used to identify or exclude this as a cause.
Preparing for Your Colonoscopy
Good bowel preparation is essential — if the bowel is not clean, the colonoscopy may need to be repeated. Follow the instructions below carefully. You will also receive written instructions from our team after your appointment is confirmed.
2 Days Before — Start a Low-Fibre Diet
Stop eating high-fibre foods. Avoid whole grains, brown rice, lentils (dal), raw vegetables, nuts, seeds, and most fruits. Stick to white rice, white bread, eggs, chicken, fish, curd, and boiled potatoes.
Day Before — Clear Liquid Diet + Bowel Prep
Eat nothing solid from the morning of the day before. Drink only clear fluids: plain water, coconut water, clear broth (no fat), black tea or coffee (no milk), apple juice, sports drinks (Glucon-D, Electral). Begin the prescribed bowel preparation solution as directed — usually in two doses, afternoon and evening.
Morning of the Procedure — Nil by Mouth
Do not eat or drink anything (including water) for at least 4 hours before your procedure. If a second dose of bowel preparation was prescribed for the morning, take it as instructed and allow at least 2 hours after completing it before your appointment.
Medications — What to Continue and What to Pause
Most regular medications can be taken as usual with a small sip of water. However, blood thinners (aspirin, warfarin, clopidogrel, rivaroxaban, dabigatran), iron supplements, and diabetes medications may need adjustment — inform the team when booking and again during the pre-procedure check.
What to Bring
Bring your hospital registration documents, ID, insurance card, a list of your current medications, and loose comfortable clothing. Remove nail polish and jewellery. Leave valuables at home.
Plan for 4–5 Hours at the Hospital
The colonoscopy itself takes 20–45 minutes, but your total time at the hospital will be approximately 4–5 hours — including registration, pre-procedure assessment, IV placement, the procedure, and a monitored recovery period before discharge. In some cases, insurance companies require a 24-hour admission — our team will advise you at the time of booking if this applies to your policy. Do not plan any work or commitments for the rest of the day.
Arrange Transport Home
You will receive conscious sedation during the procedure and must not drive, cycle, or operate machinery for at least 6 hours afterwards. Please bring a responsible adult who can accompany you home. You should not come alone.
What You Can and Cannot Eat — Quick Reference
| Food Group | ✓ Allowed (Low-Fibre Days) | ✗ Avoid |
|---|---|---|
| Grains | White rice, white bread, plain crackers, semolina (suji) | Brown rice, whole wheat, oats, millet (bajra, jowar), poha |
| Protein | Eggs, chicken (no skin), fish, plain paneer | Dal, rajma, chhole, whole pulses, beans |
| Dairy | Curd (small amount), plain milk, plain chhach | Butter, cream, high-fat cheese |
| Vegetables | Peeled boiled potato, peeled zucchini (small amounts) | All raw vegetables, salad, bhindi, spinach, peas, cauliflower |
| Fruit | Ripe banana (small), melon without seeds, canned fruit (no pulp) | All raw fruits with skin/seeds, guava, apple, papaya, berries |
| Drinks | Water, coconut water, clear broth, black tea/coffee, apple/grape juice (strained, no pulp) | Milk, lassi, fruit with pulp, alcohol, carbonated drinks (day before) |
Drinking the bowel preparation solution: It can be unpleasant to drink in large quantities. Chill it in the refrigerator, use a straw, and follow each glass with a small sip of clear juice or sucking on a hard candy (clear/white). If you feel nauseous, slow down or pause for 15–20 minutes, then continue. Do not stop altogether without calling us first.
What Happens During the Procedure?
A colonoscopy is a day-procedure and most patients go home the same day. Here is a step-by-step guide to what happens from when you arrive at hospital to when you leave.
Arrival and Registration (30–45 minutes before)
You will be admitted to the day-procedure unit. A nurse will check your identification, confirm your procedure, record your vital signs, and review your medications and allergy history. Please inform the team of any changes to your health since booking.
IV Line and Pre-Procedure Assessment
A small intravenous (IV) cannula is placed in the back of your hand or forearm. The anaesthesiologist or nurse anaesthetist will see you to discuss and administer sedation. A consent form will be reviewed if not already signed.
Sedation
Colonoscopy in India is performed under conscious sedation — not general anaesthesia. Intravenous sedation is given through the cannula, most commonly a combination of a sedative (midazolam) and a painkiller (pethidine or fentanyl). You remain conscious but deeply relaxed, feel no significant pain, and most patients have little or no memory of the procedure. You breathe entirely on your own and do not need a breathing tube. This is different from general anaesthesia — you are not fully unconscious, but you are comfortable and unaware of what is happening. In some patients, deeper sedation with propofol (monitored anaesthesia care / MAC) may be used.
Colonoscope Insertion and Advancement
You lie on your left side, knees bent. The colonoscope is gently inserted through the anus and carefully advanced through the entire large bowel to the cecum (and terminal ileum where possible). Air or carbon dioxide is used to gently inflate the bowel for a clearer view. The insertion phase typically takes 5–15 minutes depending on the length and anatomy of your colon.
Withdrawal and Inspection
The most important phase — the doctor slowly withdraws the scope, carefully inspecting every part of the bowel lining. A minimum withdrawal time of 6 minutes is a recognised quality standard. Any polyps, inflamed areas, or other abnormalities are assessed, photographed, and treated as needed. This phase takes 6–20 minutes depending on findings.
Recovery
After the procedure you are moved to the recovery area and monitored while the sedation wears off. You will be offered water and biscuits. Most patients are ready to go home within 30–60 minutes. Dr. Kapoor or a member of the team will speak to you (and your companion) to explain what was found, what was done, and what the next steps are.
Polypectomy — Removing Polyps During Colonoscopy
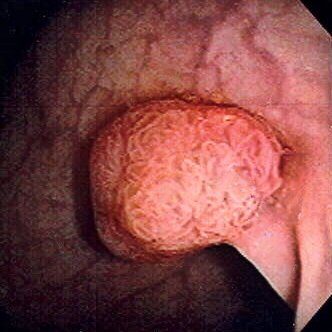
A polyp is a small growth on the inner lining of the bowel. Most polyps are benign (non-cancerous), but some types — called adenomas — can develop into cancer over many years if left untreated. Removing polyps when they are found (polypectomy) is one of colonoscopy's most powerful benefits.
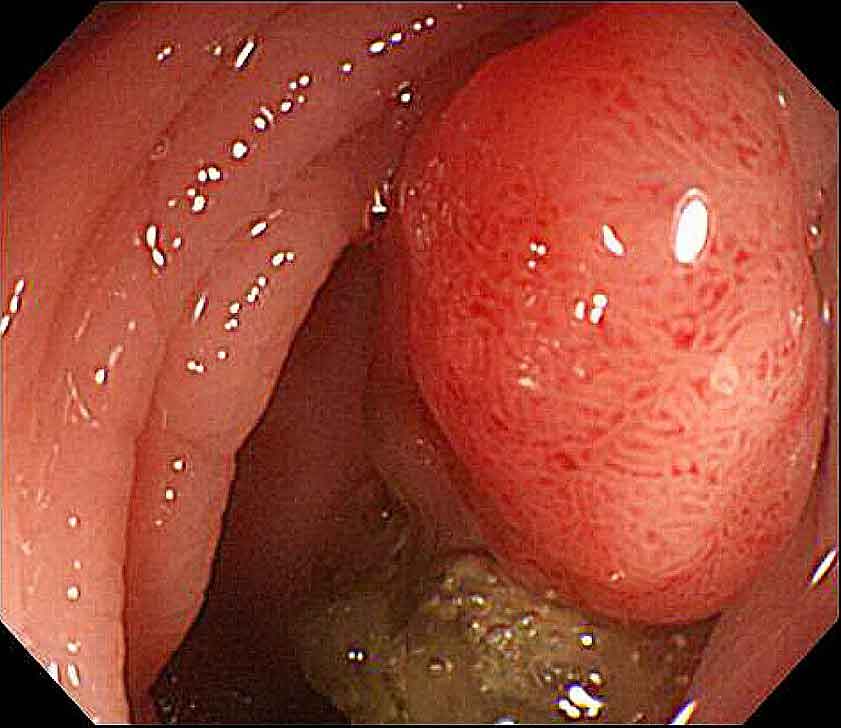
During colonoscopy, if a polyp is found, it can usually be removed at the same time — without any need for separate surgery or anaesthesia.
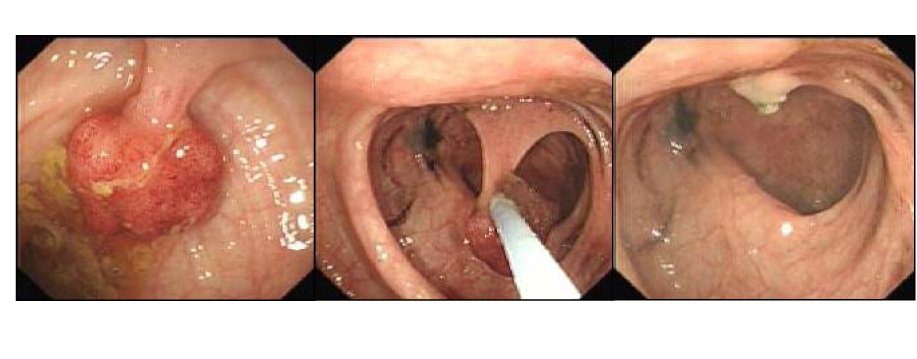
Methods of Polypectomy
- Forceps biopsy / cold biopsy: Small polyps (under 5 mm) can be grabbed and removed using biopsy forceps in one or two bites. No heat or electricity involved.
- Cold snare polypectomy: A wire loop is passed around the polyp and closed to cut it off — no electrical current used. This is now the preferred method for most small-to-medium polyps (5–20 mm) due to low bleeding risk.
- Hot snare polypectomy: Similar to cold snare, but with electrical current (diathermy) to cut and seal the stalk. Used for larger polyps or polyps with a stalk.
- Endoscopic mucosal resection (EMR): For large flat or sessile polyps, fluid is injected under the polyp to lift it, and it is then removed in pieces using a snare. Requires more skill and may need follow-up colonoscopy to check for complete removal.

Procedures Performed During Colonoscopy
A colonoscopy is not only a diagnostic tool — it is also a therapeutic one. Several procedures can be performed at the same time, avoiding the need for separate surgery or a return visit. This is one of colonoscopy's most important advantages over other bowel investigations.
Polypectomy
Removes polyps using forceps or snare — prevents colorectal cancer.
Know More
Removal using forceps, cold snare, or hot snare — depending on size and type. This prevents colorectal cancer by eliminating pre-cancerous lesions before they progress.
Biopsy
Tissue samples sent to pathology — results in 7–14 days.
Know More
Small tissue samples are taken from abnormal areas using biopsy forceps and sent to the pathology laboratory. Results help diagnose colitis, Crohn's disease, cancer, intestinal TB, and dysplasia.
Haemostasis — Control of Bleeding
Active bowel bleeding stopped using clips, diathermy, or adrenaline injection.
Know More
Active bleeding from the bowel lining can be stopped during colonoscopy using thermal energy (diathermy/electrocoagulation), metal haemoclips, injection of adrenaline, or a combination — avoiding emergency surgery in many cases.
Argon Plasma Coagulation (APC)
Non-contact energy treatment for angiodysplasia, flat lesions, and residual polyp tissue.
Know More
Uses ionised argon gas to deliver electrical energy to abnormal tissue. Treats flat lesions, angiodysplasia (abnormal blood vessels causing bleeding), and ablates residual polyp tissue after removal.
Endoscopic Mucosal Resection (EMR)
Removes large flat polyps too big for standard snare polypectomy.
Know More
Fluid is injected beneath the lesion to lift it away from the muscle layer, then removed in one or multiple pieces using a snare. EMR allows removal of lesions that are too large for standard polypectomy.
Stricture Dilation
Narrowed colon segments widened using a balloon — relieves obstruction without surgery.
Know More
Narrowed segments from Crohn's disease, post-surgical scarring, or radiation can be gently widened using a balloon dilator passed through the colonoscope, relieving obstructive symptoms without surgery.
Stent Insertion
Metal stent placed across a blocked colon — relieves obstruction immediately.
Know More
A self-expanding metal stent is placed across a blocked segment — most commonly from colorectal cancer. The stent relieves the blockage immediately and can be a bridge to planned surgery, or used for palliation in advanced disease.
Decompression of Volvulus
Colonoscope passed past the twist to decompress sigmoid volvulus — avoids emergency surgery.
Know More
Sigmoid volvulus — the colon twisting on itself causing obstruction — can often be treated by passing the colonoscope past the twist to decompress the bowel. A potentially life-saving procedure that avoids emergency surgery in most cases.
Tattooing (India Ink Marking)
Ink mark placed next to a lesion to guide the surgeon during later laparoscopic surgery.
Know More
A small injection of sterile ink is placed in the bowel wall next to a polyp or lesion. This marks the location precisely so that during laparoscopic surgery the surgeon can identify the exact site from outside the colon — avoiding the need to open the entire bowel.
What to Expect After the Procedure
Most patients recover quickly from a colonoscopy. Here is what is normal and what to watch for after you go home.
Bloating and Wind (Normal)
Air or gas used to inflate the bowel during the procedure can cause bloating, cramping, or the urge to pass wind for several hours after. This is completely normal and will resolve on its own. Walking around can help.
Small Amount of Blood (Normal After Polypectomy)
A small streak of blood in the stool for 1–2 days after polypectomy is expected and not alarming. The polypectomy site heals like a small wound. If you had only biopsies taken (no polyp removal), there should be minimal if any bleeding.
Drowsiness From Sedation (Normal)
You may feel sleepy, foggy, or slightly unsteady for several hours after sedation. This is why you cannot drive or make important decisions for at least 6 hours after the procedure. Rest at home and resume normal activities the following day.
Eating and Drinking After
You may drink water and eat a light meal as soon as you feel ready — usually within 1–2 hours of returning home. Start with easily digestible foods: khichdi, dal, toast, curd, soup. Avoid heavy, spicy, or oily food on the day of the procedure.
Resuming Medications
Resume your regular medications with a normal meal unless instructed otherwise. If blood thinners (anticoagulants or antiplatelets) were paused before the procedure, the team will advise specifically when to restart them — this depends on whether a polypectomy was performed.
Return to Normal Activities
Most patients return to work and normal activities the day after their colonoscopy. Avoid strenuous exercise, heavy lifting, and alcohol for 24 hours. If a polypectomy was performed, avoid intense physical exertion for 1 week.
⚠️ Seek Urgent Medical Attention If You Experience:
- Heavy or persistent rectal bleeding (bright red blood that does not settle, or clots)
- Severe or worsening abdominal pain that is not relieved by passing wind
- Fever above 38°C with chills or rigors
- Abdominal swelling, rigidity, or hardness
- Difficulty breathing or chest pain
- Fainting or feeling faint
- Inability to pass stool or wind after 24 hours with abdominal distension
If any of these occur, go to the nearest emergency department or call Dr. Kapoor's team immediately. Do not wait until the next scheduled appointment.
Risks and Benefits
Colonoscopy is a safe procedure, and for most patients the benefit of an accurate diagnosis — or the reassurance of a normal result — far outweighs the risks. Understanding both helps you make an informed decision.
✓ Benefits
- Most accurate test for examining the entire large bowel
- Can diagnose and treat in the same procedure (polyp removal, biopsy)
- Prevents colon cancer by removing pre-cancerous polyps before they become malignant
- Detects cancer at an early, curable stage
- Provides definitive answers to symptoms like bleeding, change in bowel habit, and anaemia
- If normal, provides 10-year reassurance for average-risk individuals
- Guides treatment decisions in IBD (Crohn's disease, ulcerative colitis)
⚠ Risks (uncommon)
- Perforation (tear in the bowel wall): approximately 1 in 1,000 procedures. Higher if large polyps removed. Usually requires hospital admission and surgery.
- Bleeding after polypectomy: 1–2 in 100 polypectomies. Usually minor and stops on its own. Rarely requires re-scope or hospital admission.
- Missed lesion (incomplete examination): No test is 100% accurate. Small flat polyps and lesions behind folds can occasionally be missed.
- Reaction to sedation: Uncommon. The anaesthetic team monitors you closely throughout.
- Infection: Very rare. Sterile technique is used for all instruments.
- Incomplete procedure: Occasionally the scope cannot reach the cecum due to colon anatomy or poor preparation. CT colonography or repeat colonoscopy may be needed.
Conditions Diagnosed & Managed by Colonoscopy
Colonoscopy is the primary investigation for a wide range of colorectal and intestinal conditions. Below is a reference guide to the conditions for which it is most commonly used — for diagnosis, biopsy, treatment, or surveillance.
Colorectal Cancer — Colon & Rectum
Definitive investigation for diagnosis and biopsy of colon and rectal cancers.
Know More
Colonoscopy is the definitive investigation for diagnosis, biopsy, and staging of cancers of the colon and rectum. Early detection at colonoscopy — before the tumour causes symptoms — dramatically improves outcomes.
Learn more →Colorectal Cancer Screening
Detects cancer at its most curable stage — recommended from age 45.
Know More
Colonoscopy every 10 years from age 45 (average risk) or earlier in high-risk individuals detects cancer at its most curable stage and removes pre-cancerous polyps before they progress.
Learn more →Hereditary Polyposis — FAP & Lynch Syndrome
High-risk syndromes requiring surveillance colonoscopy, often from teenage years.
Know More
Familial Adenomatous Polyposis (FAP) and Lynch Syndrome (HNPCC) carry a very high lifetime risk of colorectal cancer. Regular surveillance colonoscopy — from teenage years in FAP — is the cornerstone of management for affected families.
Colorectal Polyps
Pre-cancerous growths detected and removed at the same procedure.
Know More
Adenomatous polyps (adenomas) are pre-cancerous growths on the bowel lining. Colonoscopy detects and removes them in the same procedure. The type, size, and number of polyps found determines the interval for surveillance colonoscopy.
Surveillance & Follow-Up Colonoscopy
Repeat at 1, 3, or 5 years after polypectomy, cancer surgery, or in IBD.
Know More
After polypectomy, colonoscopy is repeated at 1, 3, or 5 years depending on pathology results. Surveillance colonoscopy is also used after colorectal cancer surgery, in IBD to screen for dysplasia, and in hereditary syndromes.
Ulcerative Colitis (UC)
Assesses extent and severity; monitors treatment response and dysplasia surveillance.
Know More
Colonoscopy with biopsy is essential for diagnosis, assessment of disease extent (proctitis → pancolitis), monitoring response to treatment, and dysplasia surveillance in long-standing disease.
Crohn's Disease
Ileocolonoscopy assesses mucosal involvement, strictures, and fistula openings.
Know More
Ileocolonoscopy (colonoscopy + terminal ileum intubation) is the investigation of choice in Crohn's disease — assessing mucosal involvement, strictures, fistula openings, and disease activity. Biopsy confirms diagnosis and guides therapy.
Microscopic Colitis
Normal-appearing mucosa on scope — diagnosis made exclusively by biopsy.
Know More
Collagenous colitis and lymphocytic colitis cause chronic watery diarrhoea with a completely normal-appearing mucosa at colonoscopy. Diagnosis is made exclusively by biopsy — colonoscopy is both the investigation and the diagnostic tool.
Intestinal Tuberculosis
Important differential in India — biopsy distinguishes TB from Crohn's disease.
Know More
TB of the bowel is an important differential in India — particularly in the ileocaecal region — and closely mimics Crohn's disease. Colonoscopy with biopsy (for AFB, culture, and histology) is essential for accurate diagnosis and to avoid incorrect treatment.
Amebic Colitis
Characteristic flask-shaped ulcers confirmed by biopsy when stool exam is inconclusive.
Know More
Entamoeba histolytica infection causes colitis ranging from mild to fulminant. Colonoscopy demonstrates characteristic flask-shaped ulcers, most prominent in the caecum and ascending colon. Biopsy confirms the diagnosis when stool examination is inconclusive.
Ischemic Colitis
Segmental bowel inflammation from impaired blood supply — confirmed by colonoscopy.
Know More
Bowel ischaemia from impaired blood supply produces a distinctive endoscopic appearance — segmental inflammation, oedema, and haemorrhage, usually at the splenic flexure or sigmoid. Colonoscopy with biopsy confirms the diagnosis and excludes other causes.
Radiation Proctitis & Colitis
Complication of radiotherapy — bleeding vessels treated with APC at colonoscopy.
Know More
A recognised complication of radiotherapy for prostate, cervical, and rectal cancers. Colonoscopy identifies the extent of mucosal damage and allows treatment of bleeding vessels using Argon Plasma Coagulation (APC) — often avoiding blood transfusion.
Diverticular Disease
Identifies diverticula, controls bleeding, and excludes coexisting cancer.
Know More
Colonoscopy confirms the presence and extent of diverticula, identifies the source of diverticular bleeding, and excludes coexisting polyps or cancer. Haemostasis at colonoscopy can control active diverticular bleeding without surgery.
Colorectal Stricture
Narrowing assessed — balloon dilation and biopsy at the same sitting.
Know More
Narrowing of the colon or rectum — from Crohn's disease, post-surgical scarring, radiation, or cancer — can be assessed and treated at colonoscopy. Balloon dilation and biopsy can be performed in the same sitting.
Sigmoid Volvulus
Colonoscopic decompression is both diagnostic and avoids emergency surgery.
Know More
Twisting of the sigmoid colon causes acute large-bowel obstruction. Colonoscopic decompression — passing the scope past the twist to deflate the bowel — is both diagnostic and therapeutic, and avoids emergency surgery in the majority of cases.
Angiodysplasia & Vascular Ectasia
Abnormal blood vessels causing GI bleeding — identified and treated with APC in one session.
Know More
Abnormal, dilated blood vessels in the bowel lining are a common cause of lower GI bleeding — particularly in older patients. Colonoscopy identifies and treats them in a single session using Argon Plasma Coagulation (APC).
Solitary Rectal Ulcer Syndrome (SRUS)
Often misdiagnosed — biopsy at colonoscopy provides the definitive diagnosis.
Know More
A benign but often misdiagnosed condition causing rectal bleeding, mucous discharge, and straining. Colonoscopy reveals a characteristic ulcer or polypoid lesion on the anterior rectal wall; biopsy provides the definitive diagnosis.
Faecal Incontinence
Excludes structural causes before anorectal physiology testing.
Know More
Colonoscopy is used to exclude structural causes of incontinence — rectal prolapse, rectal tumour, proctitis, or radiation damage — before proceeding to anorectal physiology testing and sphincter imaging.
Recto-Vaginal Fistula
Identifies internal opening, assesses mucosal disease, and guides surgical planning.
Know More
An abnormal communication between the rectum and vagina causing faecal or gas passage through the vagina. Colonoscopy identifies the internal opening, assesses mucosal disease (Crohn's, radiation, malignancy), and guides surgical planning.
Learn more →Colovesical Fistula
Identifies colonic fistula, excludes malignancy, and assesses bowel disease before surgery.
Know More
An abnormal tract between the colon and urinary bladder — most commonly from diverticular disease or Crohn's disease. Colonoscopy identifies the colonic side of the fistula, excludes malignancy, and assesses the underlying bowel disease before surgery.
Colo-Vaginal Fistula
Assesses internal opening and mucosal extent before definitive surgical repair.
Know More
Communication between the colon and vagina — typically from diverticular disease, post-surgical complication, or Crohn's disease. Colonoscopy assesses the internal opening, mucosal disease extent, and helps plan definitive surgical repair.
Frequently Asked Questions
Is colonoscopy painful?
Most patients receive sedation (intravenous medicines) before the procedure, so they feel little or no discomfort during the colonoscopy. Some mild bloating or cramping may occur after the procedure as the air introduced during the examination passes out. The vast majority of patients describe the preparation as the most uncomfortable part — not the procedure itself.
How long does a colonoscopy take?
The colonoscopy procedure itself typically takes 20–45 minutes. However, including preparation, sedation, the procedure, and recovery before discharge, plan for a total hospital visit of 4–5 hours.
Can I eat or drink before a colonoscopy?
You will need to follow a low-fibre diet for 1–2 days before the procedure and a clear liquid diet on the day before. You must consume a prescribed bowel preparation solution to empty the colon. Nothing should be eaten or drunk (including water) for at least 4 hours before the procedure. If a morning dose of bowel preparation was prescribed, finish it at least 2 hours before your appointment time.
What is polypectomy and is it done at the same time?
A polypectomy is the removal of polyps (small growths) found on the lining of the colon during a colonoscopy. In most cases, polyps can be removed at the time of the colonoscopy itself using a wire loop or forceps — no separate procedure or anaesthesia is needed. The removed tissue is sent to a laboratory for microscopic examination.
When do I need a colonoscopy?
A colonoscopy may be recommended if you have rectal bleeding, a change in bowel habits lasting more than 3–4 weeks, unexplained iron-deficiency anaemia, persistent abdominal pain, or a family history of colon cancer or polyps. Routine screening colonoscopy for average-risk individuals is recommended from age 45. If you have had polyps before, you will need regular surveillance colonoscopies. Visit our Screening & Prevention page for detailed guidelines.
Can I drive home after a colonoscopy?
No. Because sedation is used, you must not drive, operate machinery, or sign legal documents for at least 6 hours after the procedure. Please arrange for a responsible adult to accompany you home. Taxis and auto-rickshaws are acceptable if a companion accompanies you, but you must not travel alone.
How often should I have a colonoscopy?
For a normal result with no polyps found, a repeat colonoscopy is recommended in 10 years for average-risk individuals. If small tubular adenomas were removed, the interval is 3–5 years. If advanced polyps (large, villous, or high-grade dysplasia) were found, or if you have a first-degree relative with colorectal cancer, the interval is usually 1–3 years. Your follow-up interval will be specified in your discharge letter.
What are the risks of colonoscopy?
Colonoscopy is a safe procedure. Serious complications are uncommon. They include a small risk of perforation (a tear in the bowel wall, occurring in approximately 1 in 1,000 procedures) and bleeding after polypectomy (1–2 in 100 polypectomies). The risk of sedation-related complications is also low. Your surgeon will discuss the specific risks relevant to your individual case at your pre-procedure consultation.
