
Colorectal Cancer
Understanding cancer of the colon and rectum — what it is, how it is found, and how it is treated through surgery.
& JCI
What Is Colorectal Cancer?
Colorectal cancer is cancer that starts in the large bowel (colon) or the back passage (rectum). Together, these two areas make up the large intestine — the last part of your digestive system.
Most colorectal cancers begin as small, non-cancerous growths called polyps. Over several years, some polyps can slowly turn into cancer. This is why regular colonoscopy screening is so important — catching polyps early means we can remove them before they become cancer.
Colorectal cancer is one of the most common cancers in India, and one of the most treatable when found early. With surgery, and sometimes chemotherapy or radiotherapy alongside it, many patients go on to live full, healthy lives.
Dr. Rajeev Kapoor specialises in the surgical treatment of colon cancer and rectal cancer at Fortis Hospital Mohali, with over 35 years of experience in colorectal and cancer surgery.

Signs & Symptoms
Colorectal cancer can cause a range of symptoms, though in early stages there may be none at all. This is why screening matters. If you notice any of the following, speak to a doctor.
⚠️ See a Doctor Soon
- Blood in your stools (even once)
- A persistent change in bowel habits (looser, more frequent, harder)
- Feeling that your bowel hasn't fully emptied
- Unexplained weight loss
Abdominal Symptoms
- Stomach pain or cramping
- Bloating or discomfort
- A lump or swelling in the abdomen
General Symptoms
- Tiredness and low energy
- Anaemia (low blood count)
- Loss of appetite
High-Risk Groups
- Age 50 and above
- Family history of colorectal cancer or polyps
- Inflammatory bowel disease (IBD)
- Previous colorectal polyps
How Is It Diagnosed?
Finding colorectal cancer early greatly improves outcomes. Several tests help confirm whether cancer is present and how far it has spread.
-
Colonoscopy
A thin, flexible camera is passed into the bowel to look for polyps or abnormal areas. A small tissue sample (biopsy) may be taken at the same time. This is the gold-standard test. Read about colonoscopy →
-
CT Scan & MRI
Imaging scans show how large the tumour is, whether it has spread to nearby lymph nodes, and whether it has reached other organs such as the liver or lungs.
-
Blood Tests & Tumour Markers
Blood tests including CEA (a tumour marker) and full blood count help assess your overall health and monitor for cancer activity.
-
PET Scan (if needed)
A PET scan is sometimes used to check for spread to distant sites, especially when planning surgery for recurrent or advanced cancer. What to expect from a PET scan →

Cancer Staging — What the Stages Mean
After diagnosis, the cancer is given a stage (0 to 4). The stage tells your surgeon how far the cancer has grown and helps plan the best treatment.
| Stage | What It Means | Typical Treatment Approach |
|---|---|---|
| Stage 0 | Very early — cancer cells are only in the inner lining of the bowel wall. | Removal during colonoscopy or minor local surgery. |
| Stage I | Cancer has grown into the bowel wall but has not spread to lymph nodes. | Surgery to remove the affected section of bowel (resection). |
| Stage II | Cancer has grown through the bowel wall but lymph nodes are clear. | Surgery, sometimes with chemotherapy after. |
| Stage III | Cancer has spread to nearby lymph nodes. | Surgery followed by chemotherapy. For rectal cancer, radiotherapy may be given before surgery. |
| Stage IV | Cancer has spread to other organs (commonly liver or lungs). | Surgery combined with chemotherapy, targeted therapy, or advanced cancer surgery. Each case is planned individually. |
Even Stage IV colorectal cancer can be treated and, in some cases, cured — particularly when liver or lung metastases can be surgically removed.
Surgery for Colorectal Cancer
Surgery is the main treatment for colorectal cancer. The goal is to remove the tumour with a clear margin of healthy tissue, along with the related lymph nodes. The exact operation depends on where the cancer is and how advanced it has become.
-
Right Hemicolectomy
Removal of the right side of the colon. Used for cancers in the caecum, ascending colon, or hepatic flexure. What is a right hemicolectomy? →
-
Left Hemicolectomy & Sigmoid Resection
Removal of the left colon or sigmoid (S-shaped) section. Used for cancers on the left side of the colon. About left hemicolectomy →
-
Anterior Resection (for Rectal Cancer)
The rectum is removed and the colon is joined back to the remaining bowel. In most cases, the patient keeps their normal bowel function. For rectal cancer, this is the most common operation. What to expect from anterior resection →
-
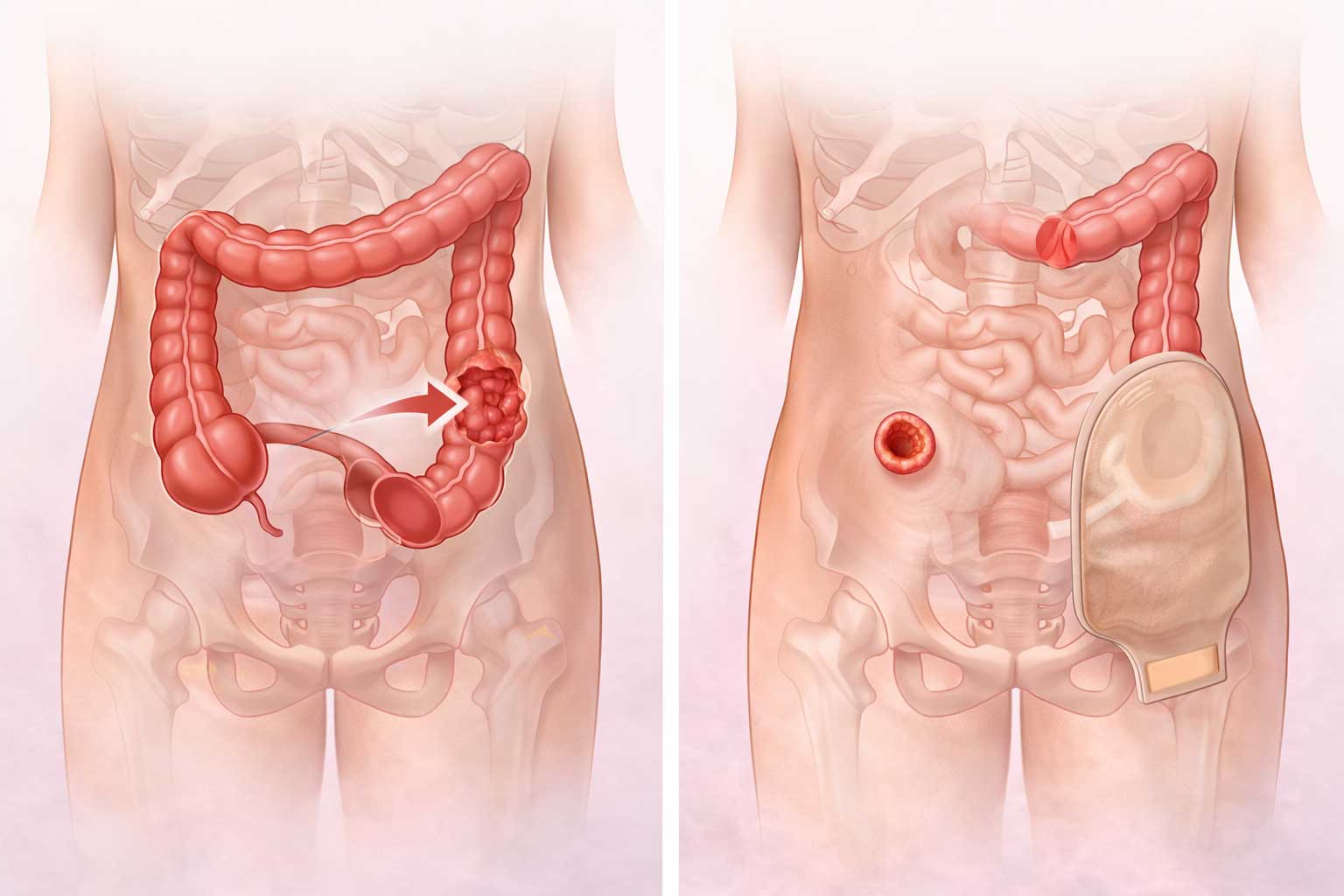
Abdominoperineal Resection (APR)
Used for very low rectal cancers. The rectum and anus are removed, and a permanent colostomy (stoma) is formed. This is only done when it is not possible to join the bowel back together. About APR surgery →
-
Total Mesorectal Excision (TME)
A precise surgical technique for rectal cancer where the rectum is removed together with all surrounding tissue in one package, reducing the risk of cancer coming back locally. This gold-standard technique is used by Dr. Kapoor for all rectal cancer operations. What is TME? →
-
Laparoscopic (Keyhole) Surgery
Most colorectal cancer operations can be done through small cuts using a camera, reducing pain, hospital stay, and recovery time. More about laparoscopic surgery →
-
Robotic Surgery (da Vinci® System)
The most advanced form of minimally invasive colorectal surgery. Using the da Vinci® robotic system, Dr. Kapoor operates with magnified 3D vision and wristed instruments that bend and rotate beyond the human hand — ideal for precise rectal cancer surgery in the narrow pelvis. Learn more about robotic surgery →
-
Liver Metastasis Surgery
When colorectal cancer has spread to the liver, surgical removal of the liver deposits is possible in selected patients and can be curative. More about cancer surgery →

Robotic Surgery for Colorectal Cancer
Robotic-assisted surgery is the most advanced form of minimally invasive surgery available today for colorectal cancer. Dr. Rajeev Kapoor performs robotic colorectal surgery at Fortis Hospital Mohali using the da Vinci® Surgical System — offering patients a safer, more precise alternative to traditional open surgery.
da Vinci® Robotic Surgical System
The da Vinci® system gives the surgeon a magnified, high-definition 3D view inside the body. Small robotic arms — controlled entirely by Dr. Kapoor — use instruments that can bend and rotate with far greater precision than the human hand. This is particularly valuable for rectal cancer operations, where the surgeon must work in the narrow confines of the pelvis.
The robot does not operate independently — it is a tool that extends the surgeon's skill and precision.

Why Robotic Surgery?
Compared to open or standard laparoscopic surgery, robotic surgery offers several important advantages for suitable patients:
Enhanced Precision
Wristed instruments with 7 degrees of freedom allow movements that are impossible with standard laparoscopic tools — reducing the risk of injury to surrounding structures.
Magnified 3D Vision
High-definition 3D camera gives a detailed, immersive view deep inside the pelvis — critical for preserving nerves that control bladder and sexual function.
Less Blood Loss
Greater surgical control means less inadvertent bleeding during dissection, reducing the chance of needing a blood transfusion.
Shorter Hospital Stay
Patients typically return home sooner after robotic surgery compared to open surgery — often within 3–5 days for colon procedures.
Faster Recovery
Smaller incisions mean less pain, fewer wound complications, and a quicker return to normal activities and work.
Nerve Preservation
Critical for rectal cancer — robotic TME allows precise nerve-sparing to protect bladder and sexual function, which matters greatly to patients' quality of life after surgery.
Open vs Laparoscopic vs Robotic Surgery
Each approach has its place. The right choice depends on the cancer location, patient health, and surgical complexity.
| Feature | Open Surgery | Laparoscopic (Keyhole) | Robotic Surgery ✦ |
|---|---|---|---|
| Incision Size | Large (15–25 cm) | Small (5–10 mm ports) | Small (5–12 mm ports) |
| 3D Surgical Vision | ✗ No | 2D only | ✓ HD 3D |
| Instrument Flexibility | Limited (human wrist) | Limited (rigid shafts) | ✓ 7° of motion (wristed) |
| Tremor Elimination | ✗ | ✗ | ✓ Built-in tremor filter |
| Blood Loss | Higher | Moderate | ✓ Minimal |
| Hospital Stay | 5–7 days | 3–5 days | ✓ 2–4 days (typical) |
| Best For | Complex / emergency cases | Colon resections | ✓ Rectal cancer, TME, narrow pelvis, revision surgery |
Which Colorectal Cancer Operations Can Be Done Robotically?
Dr. Kapoor performs the following operations using the robotic approach at Fortis Hospital Mohali: Robotic Anterior Resection (for rectal cancer), Robotic Total Mesorectal Excision (TME), Robotic Right and Left Hemicolectomy, Robotic Sigmoid Resection, and Robotic Abdominoperineal Resection (APR). The suitability of a robotic approach is assessed individually — not every patient or cancer type is suitable, and Dr. Kapoor will advise you on the best surgical method for your case.
Other Cancers Dr. Kapoor Treats
Dr. Rajeev Kapoor's expertise extends well beyond colorectal cancer. As a specialist cancer surgeon at Fortis Hospital Mohali, he also performs surgery for the following cancers — each requiring a high level of surgical skill and oncological knowledge.
Small Bowel Cancer
Rare tumours of the small intestine, including adenocarcinomas and carcinoid tumours. Surgical resection is the primary treatment. Early diagnosis is key, as these cancers are often found late due to vague symptoms.
Soft Tissue Sarcomas
Cancers arising from connective tissues — muscles, fat, nerves, or blood vessels. Abdominal and retroperitoneal sarcomas require specialist surgical expertise for complete removal and the best chance of cure.
Skin & Perianal Skin Tumours
Skin cancers in the perianal region, including squamous cell carcinoma, basal cell carcinoma, and melanoma, are managed surgically with wide local excision or more extensive resection when needed.
Vulval Cancer
Dr. Kapoor works as part of a multidisciplinary team to manage vulval cancer cases that require surgical input, including radical excision and reconstruction in collaboration with gynaecological oncology colleagues.
Anal Cancer
Surgery for anal cancer, including abdominoperineal resection for residual or recurrent disease after chemoradiotherapy.
Appendix & Peritoneal Cancers
Appendiceal tumours and peritoneal surface malignancies, including pseudomyxoma peritonei — managed with cytoreductive surgery and, where appropriate, advanced cancer surgery techniques →
If you or a family member has been diagnosed with a cancer not listed here, please contact us — Dr. Kapoor will be happy to discuss your case and guide you to the right specialist if needed.
Beyond Cancer — Other Surgeries Performed
Dr. Kapoor is a fully trained general and colorectal surgeon. In addition to cancer surgery, he performs a wide range of other operations at Fortis Hospital Mohali, covering both planned procedures and emergency care.
Hernia Surgery
Repair of inguinal (groin), incisional, umbilical, and ventral hernias using open and laparoscopic techniques with mesh reinforcement where appropriate.
Gallbladder Surgery
Laparoscopic cholecystectomy (keyhole gallbladder removal) for gallstones, cholecystitis, and related biliary conditions. More about gallbladder surgery →
Emergency & Acute Abdomen Surgery
Immediate surgery for appendicitis, bowel obstruction, perforation, and gastrointestinal bleeding. Available at Fortis Mohali around the clock.
Stoma Formation & Reversal
Creation of a colostomy or ileostomy when needed, as well as planned stoma reversal (closure) once healing is complete. Full patient education and support provided.
Benign Colorectal Surgery
Surgery for non-cancerous conditions of the large bowel — including diverticular disease, rectal prolapse, IBD-related surgery, and colonic obstruction.
Skin, Soft Tissue & Wound Surgery
Management of cellulitis, necrotising fasciitis (flesh-eating infection), abscesses, wound debridement, and split-thickness skin grafting for complex wounds and soft tissue defects.
Related Pages
For appointments or enquiries: Contact page | drrajeevkapoor.com
