Appendiceal Cancer — Symptoms, Types & Treatment
A patient guide to understanding tumours of the appendix — types, symptoms, diagnosis, and the surgical treatments available.
The Appendix & Its Conditions
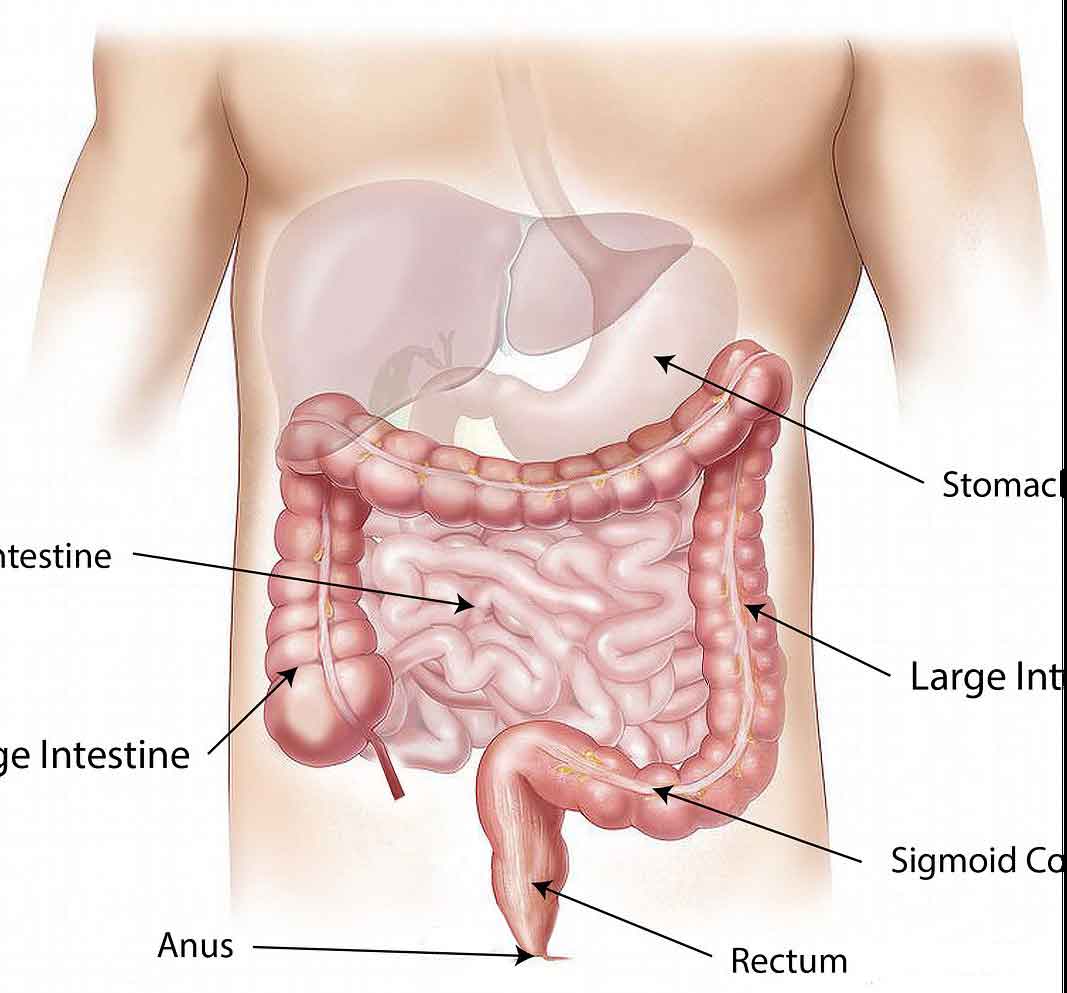
The appendix is a small, finger-shaped pouch attached to the beginning of the large bowel (the caecum) in the lower right side of the abdomen. In adults it is typically 5–10 cm long. Its exact function is not fully understood, though it may play a minor role in the immune system.
Several different conditions can affect the appendix — ranging from common inflammatory emergencies like appendicitis to rare tumours. Because the appendix is small and tucked away, many conditions here cause no obvious symptoms early on. Appendiceal tumours are often found by accident — during a colonoscopy, a CT scan done for another reason, or when the appendix is removed for what appeared to be appendicitis.
Appendiceal tumours account for roughly 0.4–1% of all gastrointestinal tumours. They cover a wide spectrum — from slow-growing neuroendocrine tumours that are usually curable, to more aggressive adenocarcinomas requiring extensive surgery.
Appendicitis
The most common appendix condition. Acute inflammation causing right lower abdominal pain — usually treated urgently by appendicectomy. Can be laparoscopic or open.
Appendiceal Mucocele
Abnormal distension of the appendix with mucus — often found incidentally on CT. Requires careful surgical removal. Rupture can lead to pseudomyxoma peritonei.
Appendiceal Tumours
A wide spectrum — from slow-growing carcinoids (usually curable) and mucinous neoplasms, to aggressive adenocarcinoma. This page covers all tumour types in detail.
Pseudomyxoma Peritonei (PMP)
Mucin spreading into the abdominal cavity after rupture of an appendiceal mucinous neoplasm. A rare but serious complication requiring specialist CRS + HIPEC surgery.
Types of Appendiceal Tumours
Several distinct types of tumour can arise in the appendix. Each has a different behaviour, and the treatment depends entirely on the type and stage found.
Neuroendocrine Tumour (Carcinoid)
The most frequently found appendiceal tumour, usually discovered incidentally after an appendicectomy. Small carcinoids (<2 cm) are almost always cured by appendicectomy alone. Larger tumours may need a right hemicolectomy. They rarely cause symptoms unless they spread to the liver.
Mucinous Neoplasms (LAMN / HAMN)
These tumours produce mucus inside the appendix, causing it to balloon (a mucocele). Low-grade appendiceal mucinous neoplasms (LAMN) behave slowly but can rupture and spread mucin into the abdomen — a condition called pseudomyxoma peritonei. High-grade mucinous neoplasms (HAMN) carry greater risk.
Appendiceal Adenocarcinoma
A true cancer of the appendix lining, this behaves similarly to colon cancer. Treatment requires right hemicolectomy and lymph node removal. If the cancer has spread to the peritoneum, HIPEC surgery may be considered. Prognosis depends on stage at diagnosis.
Goblet Cell Carcinoid / Adenocarcinoma
A mixed tumour that has features of both a carcinoid and an adenocarcinoma. It is more aggressive than a pure carcinoid and is treated like an adenocarcinoma. Right hemicolectomy is standard, and systemic chemotherapy may be recommended depending on the grade.
Pseudomyxoma Peritonei (PMP)
Not a tumour itself, but a condition caused by a ruptured mucinous appendiceal neoplasm spreading gelatinous mucin throughout the abdominal cavity. PMP grows slowly but progressively fills the abdomen. Treatment is cytoreductive surgery (CRS) combined with HIPEC at specialist centres.
Other Rare Tumours
Lymphoma, gastrointestinal stromal tumour (GIST), and sarcoma can also rarely arise in or near the appendix. These are very uncommon and require specialised multidisciplinary management including oncology input.
Appendix Neoplasms — Incidence & 5-Year Survival
*Low-grade mucinous neoplasms and villous adenomas are benign on histology but can cause pseudomyxoma peritonei if they rupture. Survival figures are approximate and vary by stage at diagnosis. Source: SEER database, published appendiceal tumour series.
Symptoms of Appendiceal Cancer
Appendiceal tumours are often silent for a long time. When symptoms do appear, they can be vague and easily mistaken for other, more common conditions. Some patients have no symptoms at all.
⚠ Symptoms That May Indicate an Appendiceal Tumour
- Dull, persistent pain in the lower right abdomen
- Bloating or a feeling of fullness in the abdomen
- A change in bowel habits — new constipation or diarrhoea
- Unexplained weight loss
- Nausea or reduced appetite
- A palpable mass in the right lower abdomen
- Increasing abdominal girth (in PMP, as mucin accumulates)
- Ascites — visible fluid accumulation in the abdomen
- Early satiety — feeling full after eating very little
- Symptoms mimicking appendicitis — acute pain, fever, vomiting
- Flushing, wheeze, or diarrhoea (carcinoid syndrome — if liver spread)
💡 Incidental discovery is common. Many appendiceal tumours are found only after appendicectomy done for apparent appendicitis. If your pathology report after appendix surgery mentions the words carcinoid, mucinous neoplasm, or adenocarcinoma, ask your surgeon about next steps immediately.
Risk Factors for Appendiceal Cancer
Appendiceal tumours are rare and can affect people with no obvious risk factors. However, certain conditions and characteristics are associated with a higher likelihood of developing them.
Age
Appendiceal cancers are most commonly diagnosed between the ages of 40 and 60, with peak incidence in the 50s. Carcinoid tumours can occur at a younger age. Risk increases with advancing age overall.
Sex
Neuroendocrine tumours (carcinoids) of the appendix are slightly more common in women. Mucinous adenocarcinoma and PMP show a similar distribution across sexes. Overall, appendiceal cancer affects men and women roughly equally.
Tobacco Use
Smoking is associated with a modestly increased risk of appendiceal neoplasms, as with many gastrointestinal cancers. Cessation of smoking reduces overall cancer risk and improves surgical outcomes.
Hereditary Conditions
Multiple endocrine neoplasia type 1 (MEN1) is associated with NETs of the appendix. Familial adenomatous polyposis (FAP) increases risk of adenomatous polyps and adenocarcinoma throughout the GI tract, including the appendix. Discuss screening if you have a hereditary cancer syndrome.
Stomach Conditions
Conditions that reduce stomach acid production — including atrophic gastritis, pernicious anaemia, and Zollinger-Ellison syndrome — have been associated with a slightly higher risk of NETs throughout the GI tract, including the appendix.
No Identifiable Risk Factor
Most patients with appendiceal tumours have no known risk factors. The majority are found incidentally — on imaging done for another reason, or when pathology is reported after appendicectomy for apparent appendicitis. Regular bowel cancer screening from age 45 is still recommended.
Diagnosing Appendiceal Cancer
Because symptoms are often absent or non-specific, most appendiceal tumours are either found incidentally or require a combination of imaging and pathology to confirm.
CT Scan of the Abdomen
The single most useful initial investigation. A CT scan can identify a dilated or abnormal appendix, a mucocele, peritoneal deposits, and whether lymph nodes or other organs are involved. It guides surgical planning.
Pathology After Appendicectomy
The most common route to diagnosis. All removed appendices are sent for histology. The pathologist examines the specimen under the microscope and reports the tumour type, grade, and whether the margins are clear — this determines whether further surgery is needed.
Blood Markers
Chromogranin A (CgA) and 5-HIAA in urine are useful for monitoring neuroendocrine tumours. CEA and CA-125 may be elevated in mucinous tumours. Tumour markers are most useful for monitoring response to treatment, not for initial diagnosis.
MRI and PET-CT
MRI gives better soft-tissue detail than CT and is used to map peritoneal deposits before CRS-HIPEC. PET-CT helps detect distant spread, particularly in high-grade tumours or goblet cell carcinomas.
Colonoscopy
A colonoscopy allows direct visualisation of the caecum, where the appendix opens. It helps rule out a caecal tumour, assess whether the appendiceal opening is involved, and take biopsies if needed.
Multidisciplinary Team (MDT) Review
Every confirmed appendiceal tumour should be discussed at a cancer MDT meeting. The team includes a colorectal surgeon, oncologist, radiologist, pathologist, and specialist nurse. This ensures the most appropriate treatment plan for your specific type and stage.
Appendiceal Cancer Treatment in Chandigarh
Treatment depends on the tumour type, its size, and how far it has spread. For most patients, surgery is the primary treatment. The type of surgery varies considerably depending on what was found. Dr. Rajeev Kapoor performs all these procedures at Fortis Hospital Mohali, serving patients from across Chandigarh, Tricity, and North India.
Appendicectomy (Appendix Removal)
For small carcinoid tumours under 2 cm, removing the appendix is curative in the vast majority of cases. This is almost always done laparoscopically (keyhole surgery), allowing quick recovery. No further surgery is needed if the margins are clear.
Right Hemicolectomy
For adenocarcinomas, goblet cell tumours, larger carcinoids (>2 cm), or any tumour where the margins are not clear after appendicectomy, a right hemicolectomy is performed. This removes the appendix, caecum, right colon, and the associated lymph nodes. It is the standard oncological operation for appendiceal cancer.
Cytoreductive Surgery (CRS) + HIPEC
For pseudomyxoma peritonei and selected appendiceal adenocarcinomas with peritoneal spread, CRS removes all visible tumour deposits from the abdominal cavity. This is followed immediately by HIPEC — heated chemotherapy washed through the abdomen to kill any remaining microscopic cells. It is a major operation performed at specialist centres.
Chemotherapy
Systemic chemotherapy may be recommended for high-grade adenocarcinoma, goblet cell carcinoma with spread, or as adjuvant (preventive) treatment after surgery. Regimens are similar to those for colon cancer — typically FOLFOX or FOLFIRI. For targeted therapy, agents such as bevacizumab, cetuximab, or panitumumab may be considered in selected cases. The decision is always made at MDT.
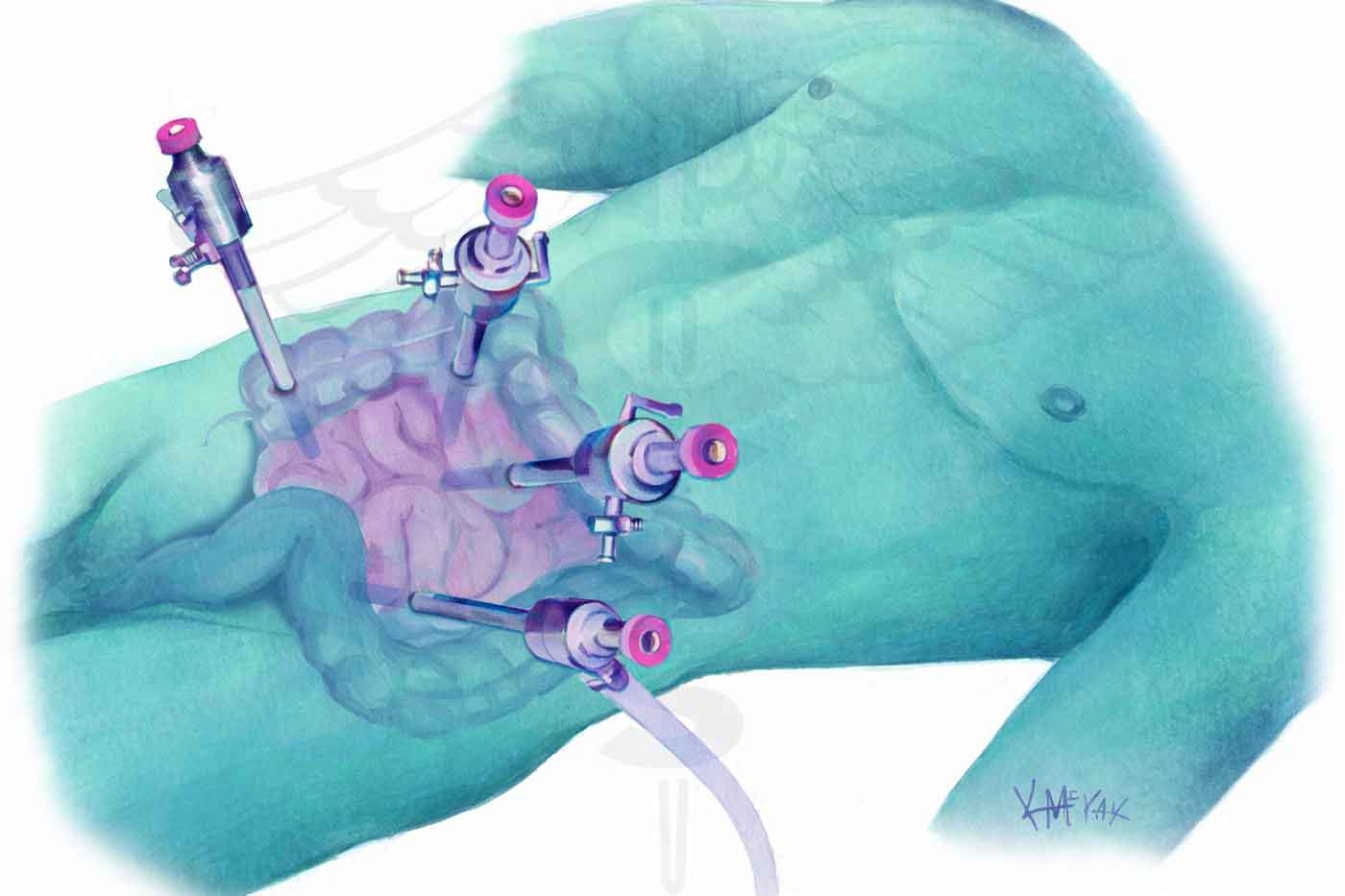
Laparoscopic (keyhole) approach — standard for appendicectomy

Removed appendix specimen sent for histology — determining the tumour type and stage
HIPEC stands for Hyperthermic Intraperitoneal Chemotherapy. It is given immediately at the end of cytoreductive surgery, while the patient is still on the operating table.

How It Works
After all visible tumour deposits have been removed, the abdominal cavity is filled with a heated chemotherapy solution (typically at 41–43 °C) and circulated through the abdomen for 60–90 minutes. The heat enhances the penetration of the chemotherapy drug into cancer cells and kills any microscopic tumour cells that remain after surgery.
Why Heated?
Cancer cells are more sensitive to heat than normal cells. The combination of direct chemotherapy contact and heat makes HIPEC significantly more effective at destroying peritoneal tumour cells than either treatment alone.
Recovery
CRS-HIPEC is a major operation typically taking 6–12 hours. Patients spend 1–2 days in intensive care and a total of 10–14 days in hospital. Full recovery at home takes several weeks. It is offered only at specialist centres with dedicated peritoneal malignancy programmes.
Is It Right for Everyone?
No. Patient selection is critical. The best candidates are those with low-volume peritoneal disease, good performance status, and no distant (liver or lung) spread. The decision is always made at a specialist MDT.
After Your Surgery — What to Expect
Recovery and follow-up depend on the operation performed. Here is a practical guide to what happens after the most common procedures for appendiceal tumours.
🏥 Hospital Stay
Laparoscopic appendicectomy: 1–2 days. Right hemicolectomy: 4–7 days. CRS-HIPEC: 10–14 days including 1–2 days in ICU. You will be up and walking the day after most operations — early mobilisation reduces complications.
🍱 Returning to Normal Activity
After a laparoscopic appendicectomy, most patients return to desk work in 1–2 weeks. After right hemicolectomy, allow 4–6 weeks. After CRS-HIPEC, full recovery typically takes 6–12 weeks. Avoid heavy lifting until your surgeon clears you.
📋 Pathology Report
The removed specimen is always sent for histopathology. Results take 7–14 days. The pathology report confirms the tumour type, grade, margins, and whether lymph nodes are involved — this determines whether further treatment is needed. Always attend your post-op clinic appointment.
📅 Follow-Up & Surveillance
After a carcinoid <2 cm: typically one CT scan at 1 year, then as needed. After right hemicolectomy or CRS-HIPEC: regular CT scans every 6–12 months for 3–5 years, tumour markers (CEA, CA 19-9), and colonoscopy at 1 year. Your surgeon will give you a personalised schedule.
⚠️ Warning Signs to Report
Contact your surgeon promptly if you develop: fever above 38.5 °C, increasing abdominal pain, wound redness or discharge, failure to pass stool or wind, or new abdominal swelling. After CRS-HIPEC, also report nausea, reduced urine output, or any new symptoms in the first 4 weeks.
🧠 Questions to Ask Your Surgeon
What type of tumour was found, and what is its grade? Were the margins clear? Were lymph nodes involved? Do I need further surgery or chemotherapy? How often will I need scans? What are the chances of recurrence? Who do I call if I am worried between appointments?
Frequently Asked Questions About Appendiceal Cancer
Other Conditions of the Appendix
Not all appendix problems are tumours. The appendix can be affected by several other conditions — some common, some rare. Understanding these helps patients make sense of their diagnosis and symptoms.

For appointments or enquiries: Contact page | drrajeevkapoor.com