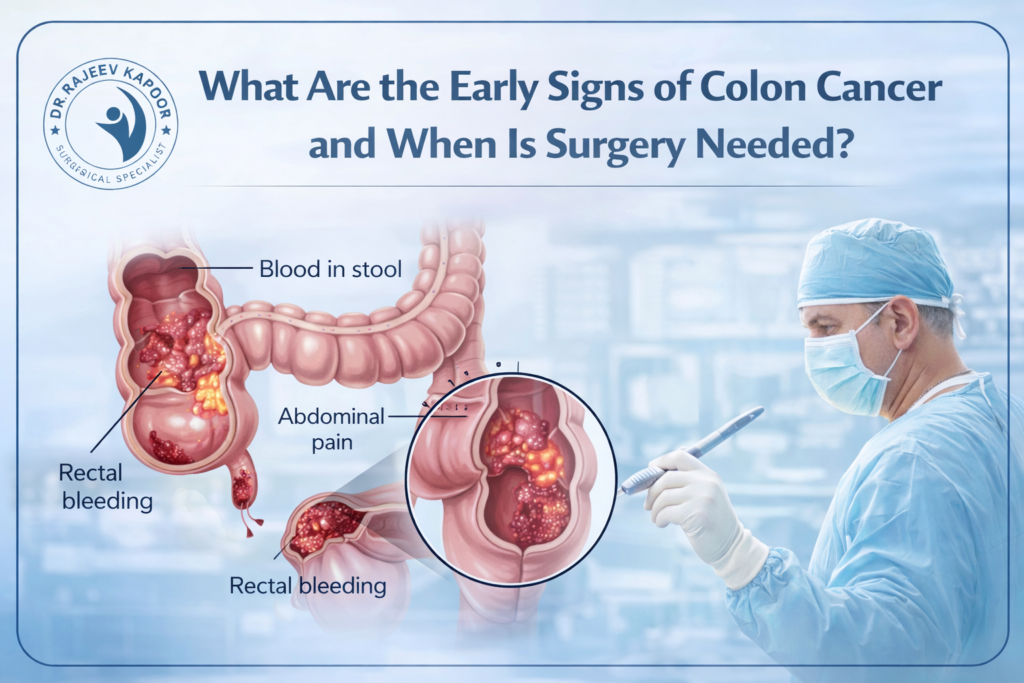
What Are the Early Signs of Colon Cancer and When Is Surgery Needed?
Colon cancer is one of the most common gastrointestinal cancers worldwide, and its incidence in India has been steadily increasing. The good news is that when detected early, colon cancer is highly treatable. With over 30 years of surgical experience, Dr. Rajeev Kapoor emphasizes early diagnosis and timely surgical intervention as the key to improving survival outcomes. This article explains the early warning signs, risk factors, and when surgery becomes necessary. What Is Colon Cancer? Colon cancer develops from the inner lining of the large intestine (colon). In most cases, it begins as a small growth called a polyp, which may gradually turn cancerous over time. Because early-stage colon cancer often produces mild or vague symptoms, it is frequently diagnosed late if screening is ignored. Early Signs of Colon Cancer Recognizing early symptoms can significantly improve outcomes. 1️⃣ Change in Bowel Habits Persistent constipation Diarrhea lasting more than a few weeks Alternating constipation and diarrhea 2️⃣ Blood in Stool Bright red blood Dark or tarry stools Occult (hidden) blood detected on testing Rectal bleeding should never be automatically attributed to piles without evaluation. 3️⃣ Persistent Abdominal Discomfort Cramping Bloating Gas Feeling of incomplete bowel evacuation 4️⃣ Unexplained Weight Loss 5️⃣ Fatigue and Weakness Chronic blood loss can lead to anemia, causing tiredness and breathlessness. If any of these symptoms persist for more than two weeks, medical evaluation is essential. Who Is at Higher Risk? Certain individuals have a higher likelihood of developing colon cancer: Age above 45 years Family history of colorectal cancer History of colon polyps Inflammatory bowel disease (ulcerative colitis or Crohn’s disease) Obesity Sedentary lifestyle High red meat, low-fiber diet Screening is especially important in high-risk individuals. How Is Colon Cancer Diagnosed? Diagnosis typically involves: Colonoscopy (gold standard test) Biopsy of suspicious lesions CT scan for staging Blood tests including tumor markers Colonoscopy not only detects cancer but can also remove precancerous polyps, preventing disease progression. When Is Surgery Needed for Colon Cancer? Surgery is the primary and most effective treatment for localized colon cancer. It is recommended when: The tumor is confined to the colon There is no distant metastasis (or limited, resectable spread) The patient develops obstruction There is persistent bleeding There is perforation Early-stage cancer treated surgically has significantly better survival rates compared to advanced disease. Types of Colon Cancer Surgery The surgical approach depends on tumor location and stage. 1️⃣ Segmental Colectomy Removal of the cancerous portion of the colon along with nearby lymph nodes. 2️⃣ Laparoscopic Colectomy Minimally invasive technique using small incisions. Benefits include: Less pain Faster recovery Shorter hospital stay 3️⃣ Open Colectomy Required for large tumors, emergency situations, or complicated cases. In some cases, a temporary or permanent stoma may be required depending on tumor location and patient condition. Is Chemotherapy Always Required? Not always. Early-stage colon cancer may require surgery alone. Stage III and some Stage II cases may need chemotherapy after surgery. Advanced disease requires a combined treatment approach. Treatment planning is individualized based on staging. Importance of Early Screening Most colon cancers develop slowly over several years. Regular screening can detect polyps before they become malignant. General recommendations: Begin screening at age 45 Earlier if there is a family history Screening methods include: Colonoscopy Stool-based tests CT colonography Early detection dramatically improves survival rates. Can Colon Cancer Be Prevented? While not all cases are preventable, risk can be reduced by: High-fiber diet Regular exercise Maintaining healthy weight Avoiding smoking Limiting alcohol intake Routine screening Prevention and early detection go hand in hand. When Should You Consult a Surgeon? Seek immediate evaluation if you experience: Persistent rectal bleeding Ongoing change in bowel habits Severe abdominal pain Symptoms of intestinal obstruction Unexplained weight loss Early surgical consultation ensures timely intervention. Conclusion Colon cancer is highly treatable when detected early. The key lies in recognizing warning signs and not ignoring persistent symptoms. Surgery remains the cornerstone of treatment for localized disease, and outcomes are significantly better when intervention occurs at an early stage. For patients considering Colon Cancer Surgery in Chandigarh, early evaluation and expert surgical management can significantly improve long-term survival.