Parastomal Hernia Treatment in Chandigarh
One of the most challenging late complications after stoma surgery — and one of the most technically demanding operations to correct. Here is what you need to know.
What Is a Parastomal Hernia?
In plain terms: A parastomal hernia — sometimes called a stoma hernia or colostomy hernia — is a bulge that forms around your stoma (the opening on your abdomen) when part of the bowel pushes through the abdominal wall. It is the most common long-term complication after stoma surgery — and it is not a sign that anything went wrong. It can happen even after a perfectly performed operation.

Up to 1 in 2 patients with a permanent colostomy develop a parastomal hernia within two years of their operation. The good news: when it is repaired by an experienced surgeon using modern techniques, outcomes are very good.
Read more
Your abdominal wall is built from layers of muscle and fibrous tissue. When a stoma is created, the surgeon makes a deliberate opening in these layers to bring the bowel to the surface. That opening — no matter how carefully made — creates a potential point of weakness. Over time, pressure from coughing, straining, or everyday movement can push tissue through this gap. That is a parastomal hernia.
It is a recognised, late complication that can develop even after a technically perfect stoma formation. It does not mean your original surgery failed.
1 in 2 people with a permanent stoma develop a parastomal hernia within 2 years

Why Does It Happen?
Several factors increase the likelihood of a parastomal hernia developing. Some are within our control at the time of surgery; others are inherent to the patient's condition.
Inherent Wall Weakness
The fascial opening created for any stoma is a structural weak point. All patients carry some baseline risk regardless of technique.
Raised Intra-abdominal Pressure
Chronic coughing, straining at stool, heavy lifting, and obesity all increase pressure on the abdominal wall around the stoma.
Previous Radiation Therapy
Pelvic or abdominal radiotherapy weakens all the tissues it passes through. Radiation-damaged fascia and skin heal poorly and have less holding strength — a major risk factor for hernia formation and for poor repair outcomes.
Malnutrition & Steroid Use
Poor nutritional status, long-term steroid therapy, and immunosuppression all impair tissue strength and healing after surgery.
Large Fascial Opening
A stoma opening that is too wide at the time of creation is a well-recognised risk factor. Too narrow, however, risks obstruction — so the surgeon must judge carefully.
Stoma Placed Off-Centre
A stoma sited away from the rectus abdominis muscle (the strong central muscle) has weaker support around it and is more prone to herniation.
Hernia risk by stoma type — maximum incidence reported in literature
Wide ranges reflect varying follow-up duration across studies. CT-detected rates are higher than clinically apparent rates.
Recognising the Problem
Parastomal hernias range from small and asymptomatic to large and functionally disabling. Not all of them require surgery immediately — but all should be assessed by a specialist.
Visible Bulge Around the Stoma
The most obvious sign — a soft swelling around the base of the stoma that often increases in size on standing or straining, and reduces when lying flat.
Poorly Fitting Appliance
As the hernia enlarges, it changes the contour of the skin around the stoma. Bags stop sealing properly, leading to leaks, skin soreness, and significant distress for the patient.
Discomfort or Dragging Pain
A heavy, dragging sensation around the stoma — especially after activity — is common. Sharp pain may signal that contents are becoming stuck (incarceration).
Obstruction or Strangulation
When bowel loops herniate and become trapped, the stoma may stop working. This is a surgical emergency. Sudden severe pain, a hard irreducible lump, and a non-functioning stoma require immediate hospital attendance.
The Unique Surgical Challenges
Parastomal hernia repair is technically demanding in ways that set it apart from ordinary hernia surgery. Several factors specific to this operation make it one of the most complex procedures in colorectal surgery.
1. Keeping the Stoma in the Same Place
After years of living with a stoma in one spot, patients know every detail of how to manage it — the position, the skin folds, the appliance routine. Moving the stoma to a new site means starting that learning process from scratch. We always aim to repair the hernia at the exact same location, without moving the stoma.
Read more
A patient with a permanent colostomy or ileostomy spends months — sometimes years — learning to manage their appliance at one specific location on their abdomen. The angle of the skin, the way it creases, the precise position relative to the belt line, the visibility in the mirror — all of this becomes deeply familiar. Patients are profoundly attached to the position of their stoma.
Moving the stoma to a new site means starting that learning process from scratch. It also means a new scar at the original site, and a significantly increased risk of incisional hernia developing there — studies show rates as high as 52% of patients who undergo stoma relocation subsequently develop a hernia at the old stoma site.
2. When Radiotherapy Was Part of Your Treatment
Many patients who need stoma surgery have also had radiotherapy for cancer. Radiation permanently changes the tissue it passes through — making skin more fragile and slower to heal. This raises the risk of complications after any repair and requires careful planning of the surgical approach and materials used.
Read more
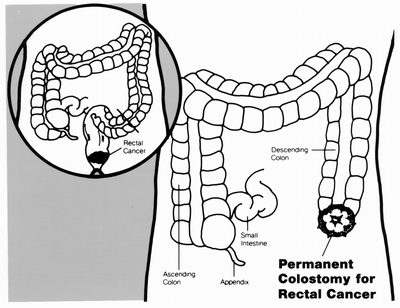
Patients who develop parastomal hernias frequently have had rectal cancer, anal cancer, or other pelvic malignancies treated with radiotherapy. Irradiated skin is thin, fragile, and slow to heal. The underlying tissue loses its strength and elasticity. Blood vessels in the radiated area are narrowed and less able to supply oxygen to healing tissue.
These changes are permanent. When operating in a previously irradiated field, wound breakdown, infection, mesh complications, and recurrence are all more likely. The choice of mesh, the depth of placement, and the surgical approach must all be tailored to the individual patient's radiation history.
3. Previous Open Abdominal Surgery
Many patients had their original bowel surgery through a large open incision — sometimes decades ago. Scar tissue inside the abdomen from that surgery makes the hernia repair more complex and time-consuming.
Read more
These patients often have extensive internal scar tissue (adhesions), large midline scars, and sometimes mesh already in place from a prior repair. The abdomen becomes a complex environment to operate in. Dissection must proceed very carefully to avoid injuring bowel stuck down by scar tissue. Operating time is longer, bleeding risk is higher, and keyhole (laparoscopic) repair may not be feasible.
4. Previous Keyhole Surgery
Having had a keyhole operation before does not make the hernia repair simple. Less scarring inside the abdomen can help — but a parastomal hernia repair is a substantial operation regardless of the approach used. Please come prepared for a full recovery.
How We Investigate
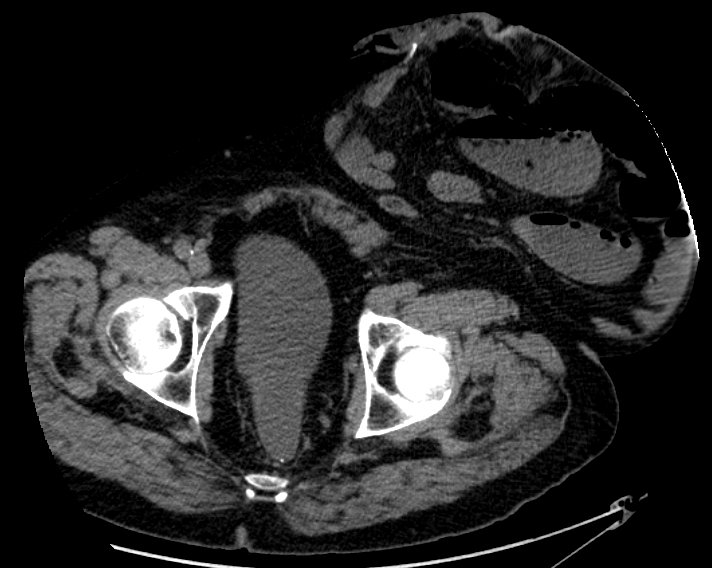
Most parastomal hernias can be diagnosed clinically — by examining the patient in the standing and lying positions. However, a CT scan is invaluable before planning repair surgery.
A physical examination — lying down and standing up — is usually all that is needed to confirm the diagnosis. A CT scan is then arranged before any surgery. The scan tells us the exact size of the hernia, what is inside it, whether there are any other hernias nearby, and whether keyhole or open surgery is safer for you.
Read more
The CT scan tells us exactly which structures are inside the hernia, the size of the fascial defect, the relationship between the bowel and surrounding vessels, and whether there are signs of partial obstruction. It directly guides the choice of surgical technique. In patients who have had radiotherapy, the scan also gives information about the condition of the surrounding tissue and any radiation-related bowel changes.
Surgical Repair Options
There is no single technique that suits every patient. The choice depends on the size of the hernia, the condition of the tissues, previous surgery and radiation history, whether the stoma can be preserved in place, and the surgeon's experience. All durable repairs today use a mesh to reinforce the closure.
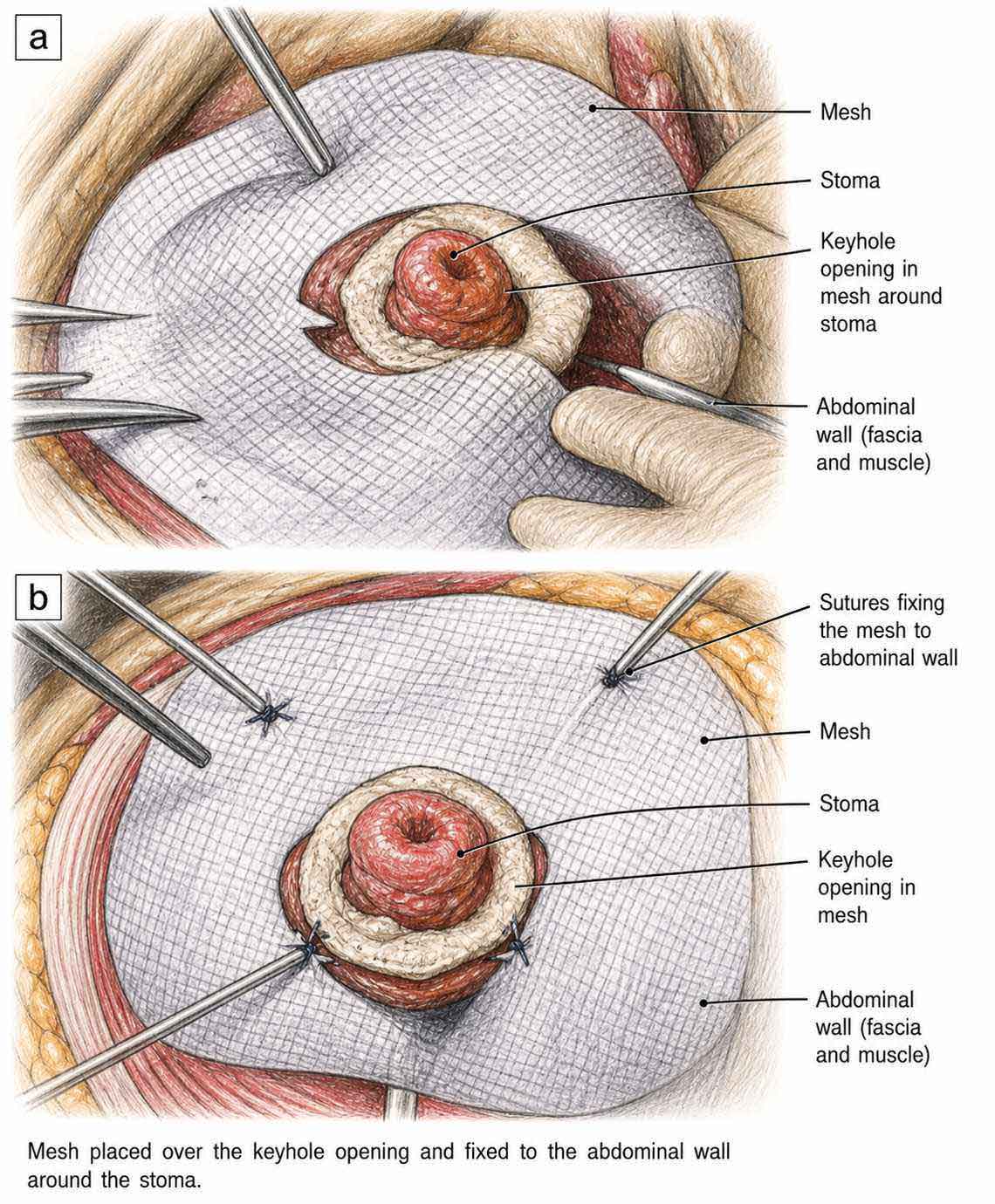
Open Mesh Repair
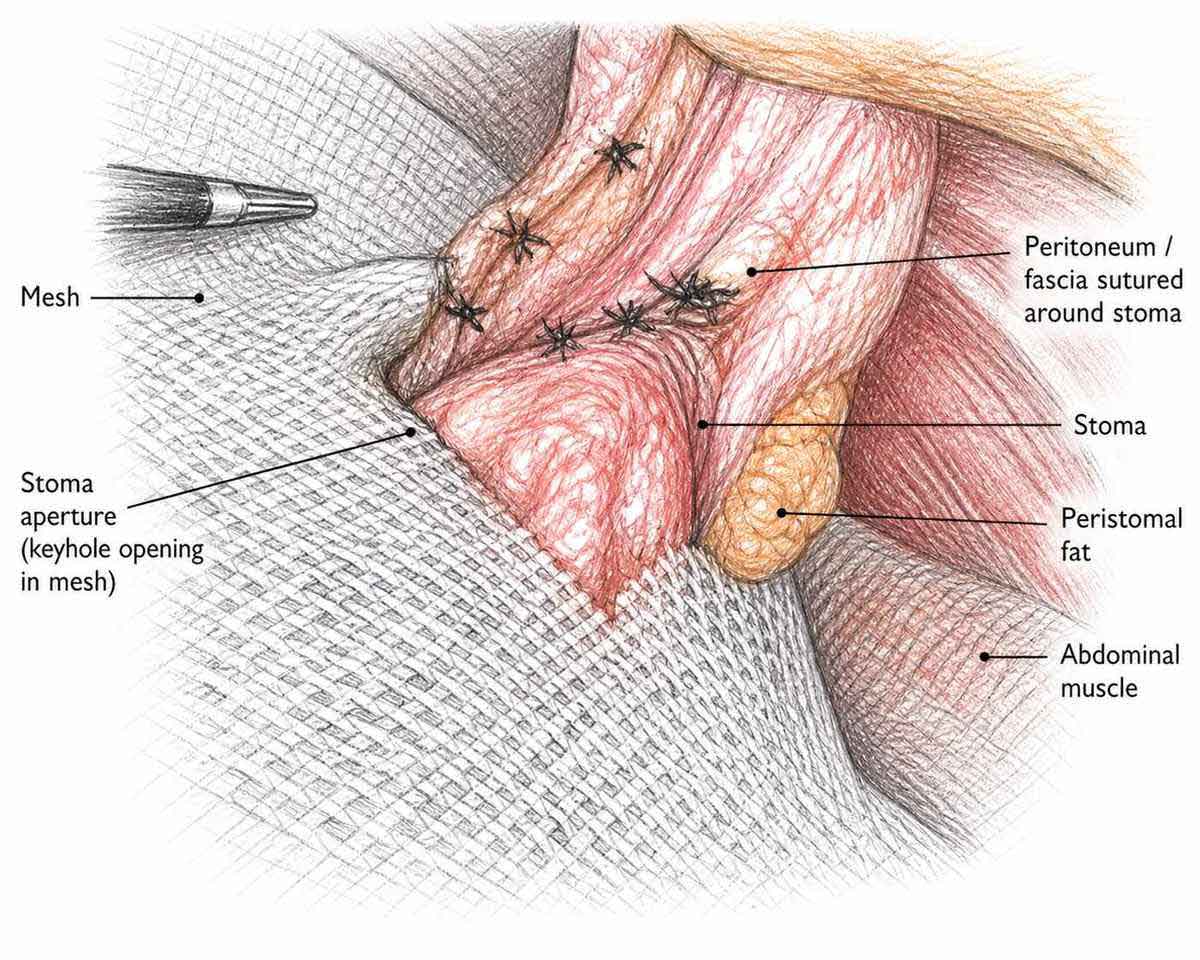
The surgeon makes a single cut in the tummy, gently returns the bulge back into the abdomen, and then narrows the opening in the abdominal wall around the stoma using sutures — making the hole the right size for the bowel to pass through comfortably. A mesh patch is then placed around the stoma to reinforce this repaired opening and hold everything in place. This is the most widely performed operation for parastomal hernia — used in roughly 8 out of 10 cases worldwide — and it is our first recommendation for most patients. Recovery is typically 4–7 days in hospital.
Read more
The hernia contents are reduced and the sac is removed. The fascial defect — the hole in the abdominal wall through which the bowel passes — is then narrowed by placing sutures around the opening to reduce its size. This step is critical: mesh placed over an unreduced defect is less durable. Once the opening is correctly sized, mesh is placed around the stoma in the retromuscular or preperitoneal plane — between the muscle layers — giving strong, durable reinforcement on all sides. This approach provides the surgeon with excellent visibility and allows careful handling of scar tissue from previous operations. Newer 3D funnel mesh designs, which seat precisely around the stoma in the retromuscular plane, have shown very good results in recent 2025 data.
Who is it for? Open repair is suitable for most patients — especially those with large hernias, dense scar tissue from previous abdominal operations, or those who are not fit enough for prolonged keyhole surgery.
Sugarbaker Technique
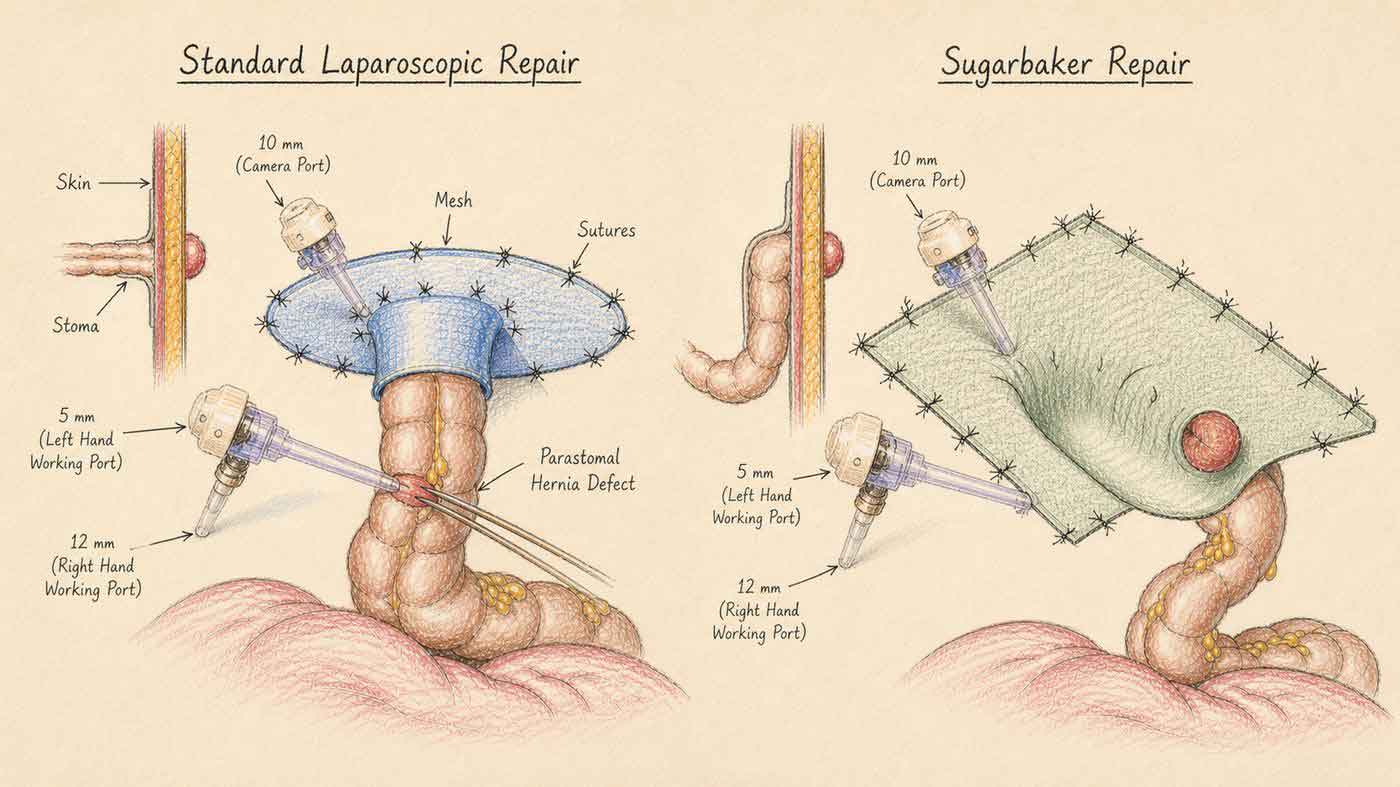
In patients fit enough for keyhole surgery, the Sugarbaker technique is the preferred keyhole option. Small cuts are made, a camera is used, and the bowel is gently tucked to one side so a wide mesh can be placed over the whole area from the inside. No large scar, and most patients go home within 2–3 days.
Read more
Unlike the standard keyhole technique, the stoma bowel is not passed through a hole in the mesh. Instead it is swept to one side and a large flat mesh covers both the defect and the bowel loop, giving more uniform reinforcement. This is particularly suited when the bowel loop is longer or comes out at a sharp angle.
Who is it for? Patients who are fit enough for a keyhole (laparoscopic) operation, have no excessive scar tissue from previous open surgery, and have a hernia of suitable size for keyhole access.
Laparoscopic Mesh Repair (IPOM)
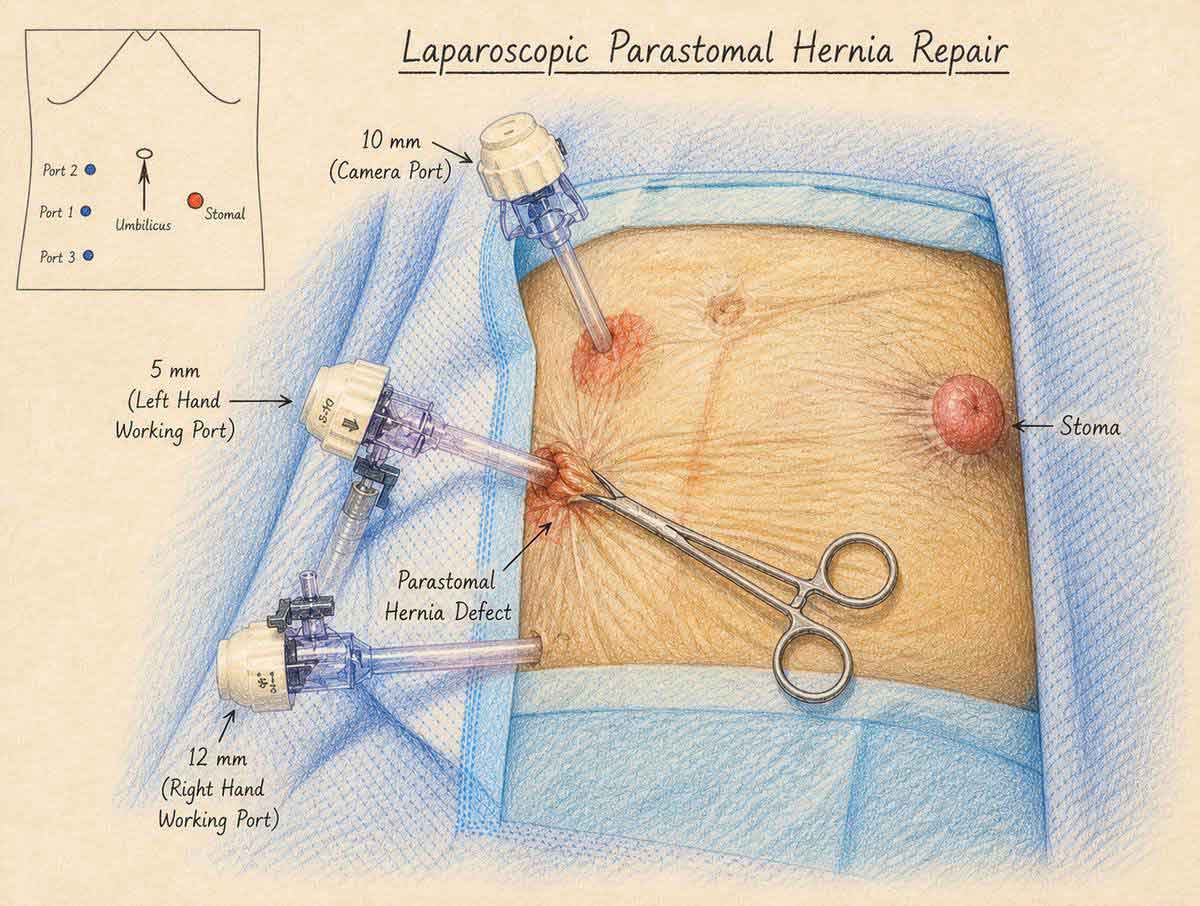
A mesh with a central opening is placed around the stoma from the inside, with the bowel passing through the centre like a key through a keyhole. Small cuts, no large scar, and most patients recover faster than with open surgery. Best suited to smaller hernias in patients who are fit for keyhole surgery.
Read more
The mesh is secured to the inside of the abdominal wall with tacks, reinforcing the area around the stoma. This technique works best when the angle between the abdominal wall and the bowel is wide and the bowel limb is relatively short. In these cases, results are very good in experienced hands.
Who is it for? Patients with smaller hernias, no major scar tissue from previous surgery, and who are fit for keyhole (laparoscopic) surgery. The Sugarbaker technique is generally preferred when keyhole surgery is chosen, but the keyhole IPOM remains an option in carefully selected cases.
Robotic Repair
In well-selected patients, the repair can be done using a robotic surgical system. The surgeon controls robotic arms from a console — the robot gives a magnified 3D view and far greater precision than standard keyhole tools, which is particularly helpful when working around the stoma in a tight space.
Read more
Robotic arms can rotate and bend inside the abdomen in ways that standard keyhole instruments cannot. This makes placing and fixing the mesh more precise, and allows more careful suturing of the abdominal wall layers. The magnified 3D view helps the surgeon identify the correct tissue planes with confidence.
Who is it for? Patients who are fit for a keyhole procedure, have a hernia of moderate size, and no extensive scar tissue from previous open surgery. Robotic repair is still emerging and is offered in specialist centres. Results so far are comparable to the best keyhole outcomes.
Sandwich Technique (Double Mesh)
Two mesh patches are placed one on top of the other — a belt-and-braces approach — for very large hernias or for hernias that have already come back after a previous repair. It is more complex than a single-mesh repair and is reserved for cases where extra reinforcement is truly needed.
Read more
A keyhole mesh is placed through the centre first, then a second wider flat mesh is placed over it in the Sugarbaker position. The double layer provides extra reinforcement across a wider area. This takes longer to perform and adds complexity, so it is only used when the clinical situation genuinely calls for it — such as a very large defect or a hernia returning after previous mesh repair.
Who is it for? Patients with very large hernias or with a hernia that has already been repaired once and has come back. Not used as a routine first-line operation.
Stoma Relocation
The stoma is moved to a different part of the tummy, leaving the hernia behind. This is only considered when it is genuinely not possible to repair the hernia at its current site. Moving the stoma means the patient has to re-learn how to manage their appliance at a completely new position — which is a significant adjustment.
Read more
After moving the stoma, the old site is closed and repaired with mesh. However, a new hernia at the old stoma site is a well-recognised complication — occurring in up to half of patients. For this reason, relocation is a last resort, used only when direct repair of the hernia is truly not feasible.
Who is it for? Patients where the anatomy, previous scarring, or other factors make repair at the original site impossible. Modern surgical techniques have reduced how often this is needed.
This older method stitches the hernia closed without mesh. Around 1 in 2 hernias come back — a recurrence rate of approximately 50%, compared to 7–17% with mesh repair. For this reason, suture repair alone is not used for planned (elective) operations.
It may be used in genuine emergencies — for example, when the bowel is obstructed and mesh cannot be safely placed at that time. In all other cases, a mesh-based technique is the standard of care.
There is no single "best" operation for parastomal hernia. The right surgery depends entirely on your situation — the size of the hernia, your general health, your previous operations, and what can be done safely.
Open surgery — through a larger cut in the tummy — is still the most common approach used worldwide, used in roughly 8 out of 10 operations. Keyhole (laparoscopic) surgery is growing but is not suitable for everyone. Your surgeon will recommend the approach that is safest and most durable for you specifically.
What the evidence says about recurrence after mesh repair
(all modern techniques)
(no mesh)
Recurrence figures are approximate and vary by follow-up duration, mesh type, and patient selection. Sources: systematic reviews and network meta-analyses 2022–2025.
How surgical practice has changed over 30 years — literature data
| Era | Stitches only (no mesh) | Open repair with mesh | Moving the stoma | Laparoscopic / Robotic |
|---|---|---|---|---|
| 1990s – early 2000s | ~28% | ~37% | ~35% | Not yet available |
| 2005 – 2015 | Falling out of use | ~80% | Reducing | ~10–12% |
| 2015 – 2025 (today) | No longer used ✕ | ~78% | Selected cases only | ~18% keyhole + 3% robotic |
Data: US National Surgical Quality Improvement Program (NSQIP) 14-year review of 73,000+ repairs; systematic reviews of 2,000+ cases; 2025 network meta-analyses.
Stoma Refashioning — Shortening the Stoma Limb
At the time of parastomal hernia repair, it is not always enough to simply reduce the hernia and reinforce the defect with mesh. Sometimes the stoma itself needs to be refashioned — and this adds another layer of complexity to an already demanding operation.
Over the years, the part of the bowel that sticks out as your stoma can become too long or floppy — and this actually makes the hernia worse by pulling on the surrounding tissue. When this happens, the surgeon shortens and reshapes the stoma at the same time as repairing the hernia.
Read more
The stoma spout can elongate or become redundant over time. A prolapsing stoma limb contributes to the hernia by pulling on the fascial edges and widening the defect. The bowel limb must be shortened by resecting the redundant segment and re-creating the stoma at the correct length.
Refashioning requires the surgeon to open the bowel, resect a segment, and create a fresh join between bowel and skin. The blood supply to the shortened stoma must be carefully preserved, and the fascial opening sized precisely — narrow enough to prevent re-herniation, but wide enough to avoid stomal obstruction or inadequate blood supply.
Mesh Choice in Refashioning Cases
When the bowel is opened during the same operation, a special type of mesh that resists infection is used instead of a standard synthetic mesh. The exact choice is made for each patient individually based on their history and the findings at the time of surgery.
Read more
Opening the bowel during refashioning creates a potentially contaminated field. Biological meshes (made from treated animal tissue) or slowly-absorbing synthetic meshes are preferred over permanent synthetic meshes in these cases, as they resist infection better. In clean cases where the bowel is not opened, standard lightweight polypropylene or composite mesh in the intraperitoneal position is appropriate.
What to Expect — Before & After
Understanding the process from assessment to recovery helps patients plan ahead and know what is normal during healing.

Before Surgery
You will be assessed in the outpatient clinic. A CT scan of the abdomen and pelvis is arranged to plan the repair. Your stoma nurse will be involved to discuss likely changes to your appliance after surgery. If you smoke or are significantly overweight, you will be asked to address this before surgery — both substantially increase complication risk. Any blood-thinning medications will need to be paused.
The Operation
Most parastomal hernia repairs are performed under general anaesthesia. The operating time depends on the approach and complexity — a straightforward laparoscopic repair may take 90–120 minutes; a complex open repair with adhesiolysis and refashioning may take considerably longer. A urinary catheter is placed during surgery. You will wake up with a new stoma bag fitted.
Recovery in Hospital
Most patients stay 2–5 days after laparoscopic repair, and longer after open surgery. Your stoma nurse will reassess the bag fit once the swelling settles. You will be helped to mobilise early to reduce clot risk. Diet is reintroduced gradually as the bowel recovers.
After Discharge
You will need 4–8 weeks of restricted activity — no heavy lifting, no strenuous exercise. Your stoma care team will follow up closely, especially if the appliance position has changed. You should be reviewed in clinic at 6 weeks and then at 3–6 months. If the hernia recurs, further options will be discussed.

Clinical Presentations & Common Questions
How a parastomal hernia presents — and what patients ask most often:
Sudden severe pain around the stoma • No stoma output for more than 6–8 hours • Skin around the stoma turning dark, blue, or purple • The hernia suddenly becomes hard and cannot be pushed back.
These are signs of strangulation or obstruction — a surgical emergency that cannot wait.
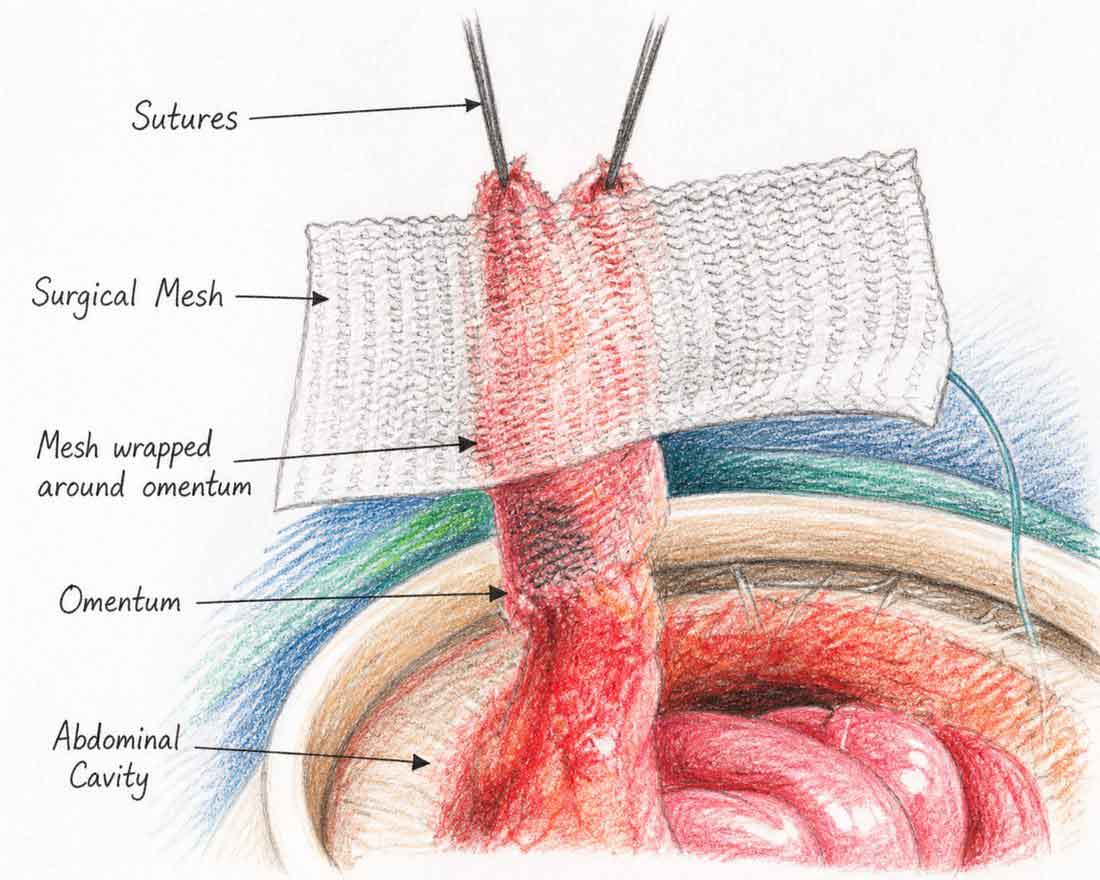
Mesh placed around the stoma — the opening in the abdominal wall is narrowed with sutures before mesh reinforcement. (AI-Generated Illustration)
Concerned About a Hernia Around Your Stoma?
Dr. Rajeev Kapoor performs all approaches to parastomal hernia repair at Fortis Hospital Mohali — including same-site repair, laparoscopic keyhole and Sugarbaker techniques, open mesh repair, and stoma refashioning. If you have a bulge around your stoma, appliance difficulties, or were told you have a parastomal hernia, an assessment is the right first step.
Contact About Dr. KapoorFor appointments or enquiries: Contact page | drrajeevkapoor.com