Gallbladder Surgery
in Chandigarh
From a silent stone found on a routine scan to complex biliary emergencies — a complete guide to gallbladder disease and its treatment.
Where Is the Gallbladder & What Does It Do?
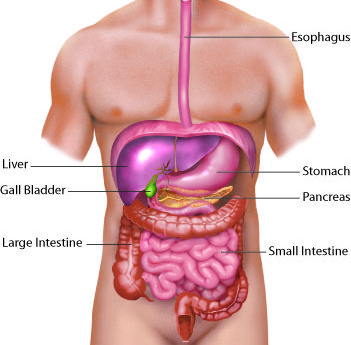
The gallbladder is a small, pear-shaped pouch tucked snugly beneath the right lobe of the liver — roughly the size of a fig. It sits just below the ribs on your right side, connected to the liver and the small intestine by a network of bile ducts.
Its job is deceptively simple: store bile. The liver manufactures bile continuously — a greenish-yellow digestive fluid that breaks down dietary fat. The gallbladder concentrates it up to tenfold and holds it in reserve, then squirts a controlled burst into the small intestine the moment you eat a fatty meal.
Between meals the gallbladder quietly fills. After meals it contracts, empties, and fills again — a cycle that repeats thousands of times over a lifetime. Most of the time this works silently and perfectly.
The gallbladder is not essential. After removal, the liver still produces bile — it simply flows directly into the small intestine at a steady trickle. The vast majority of people live completely normally without a gallbladder.
What Are Gallstones?
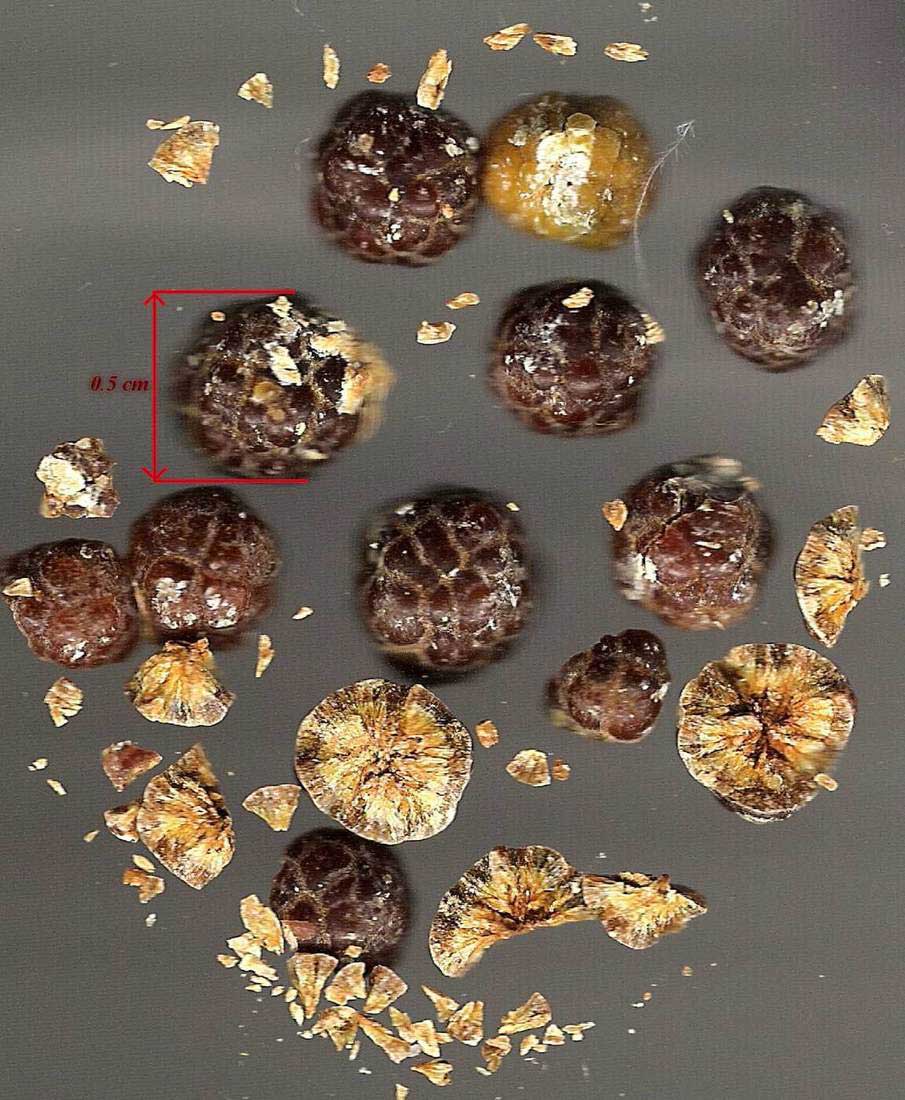
When bile chemistry tips out of balance — too much cholesterol, too little bile salts, or sluggish emptying — its dissolved components crystallise into hard deposits inside the gallbladder. These are gallstones.
Stones range from sand-sized grains to lumps the size of a golf ball. They can sit quietly for decades — or suddenly slip into the bile duct and trigger one of the most severe pain episodes a person will ever experience, without any warning.
Not every gallstone needs surgery. The decision depends on your symptoms, stone size, and overall health. Your surgeon will review each case individually — because the right treatment is rarely one-size-fits-all.
What Is a Cholecystectomy?
koh-lee-sis-TEK-toh-mee
The surgical removal of the gallbladder. It is one of the most commonly performed operations in India. You will see this word throughout this page — whenever it appears, it simply means Gallbladder Removal Surgery.
Gallstones That Cause No Symptoms
Many gallstones are discovered completely by accident — during an ultrasound done for an unrelated reason. The patient has no symptoms at all. These are called asymptomatic or silent gallstones.
Silent (Asymptomatic) Gallstones
Found on a scan for another reason — a liver check, a health screening, or an abdominal ultrasound. No pain, no nausea, no symptoms at all.
Biliary Sludge
Thick, sluggish material in the gallbladder — a mixture of micro-crystals, mucus, and calcium salts. A precursor to true stone formation. May cause no symptoms, or produce mild dyspepsia.
Gallbladder Polyps
Growths on the inner gallbladder wall, detected on ultrasound. Most are benign cholesterol polyps and can be watched with serial scans.
When is surveillance appropriate? Small asymptomatic stones (<1 cm) in a young, fit patient with a normal gallbladder may be watched. If symptoms develop, if the stones grow, or if the patient has diabetes or is about to travel to a remote area, surgery is recommended. Your surgeon will advise based on your individual picture.
When Gallstones Make Themselves Known
Symptoms begin when stones move — blocking the gallbladder outlet temporarily or irritating its wall. This can range from vague indigestion to excruciating colic.

Biliary Colic
Sudden, severe pain in the upper right abdomen — often radiating to the right shoulder or back. Triggered by fatty meals. Lasts 30 minutes to several hours, then completely settles. Recurs unpredictably. This is the hallmark symptom of gallstones.
Dyspepsia, Heaviness & Flatulence
Bloating, belching, early fullness, and vague upper abdominal discomfort after meals — particularly after fried or spicy food. Sometimes the only sign of an underperforming gallbladder. Often mistaken for acid reflux or IBS for years before stones are found.
Chronic Cholecystitis
Long-standing, low-grade inflammation from repeated stone episodes. The gallbladder wall becomes progressively thickened and scarred. Patients often describe years of vague right-sided discomfort with occasional severe attacks.
Mucocoele of the Gallbladder
When a stone blocks the gallbladder outlet without causing infection, mucus accumulates and distends the organ — producing a visibly enlarged gallbladder on ultrasound. The patient may feel a lump under the right ribs.
Gallbladder Emergencies
These conditions require same-day or emergency hospital admission. Do not wait — delay can be life-threatening.
Go to Emergency If You Have:
- Severe upper abdominal pain lasting more than a few hours — not settling with painkillers
- Fever with abdominal pain and chills (possible empyema or cholangitis)
- Yellowing of the skin or eyes (jaundice) with fever — possible cholangitis
- Sudden severe abdominal pain spreading across the whole abdomen (possible perforation)
- Vomiting you cannot control, preventing fluids
Acute Cholecystitis
A stone blocks the cystic duct and the trapped gallbladder becomes acutely inflamed. Presents with severe, constant right upper abdominal pain, fever, and tenderness.
Empyema of the Gallbladder
Pus fills the gallbladder — the most severe local complication of acute cholecystitis. The patient is toxic, with high swinging fever and severe pain.
Pericholecystic Abscess
A pocket of pus forms in the tissues surrounding the gallbladder — often walling off a small contained perforation.
Perforated Gallbladder
The end-stage complication of untreated acute cholecystitis — the gallbladder wall, under pressure from trapped infected bile, eventually gives way.
Perforation occurs in three forms: free perforation (bile spills openly into the peritoneal cavity, causing generalised peritonitis — the most dangerous); localised perforation (walled off by surrounding tissues into a pericholecystic abscess); and chronic perforation (a slow fistula into adjacent bowel). Risk is highest in elderly, diabetic, and immunocompromised patients who may present late and with blunted symptoms. The patient typically deteriorates rapidly — with diffuse abdominal rigidity, high fever, tachycardia, and shock.
Acute Gallstone Pancreatitis
When a small stone (or even sludge) slips out of the gallbladder and temporarily blocks the pancreatic outflow at the ampulla of Vater, digestive enzymes back up into the pancreas itself — triggering acute inflammation.
Gallstones are the single most common cause of acute pancreatitis in India. Presents with severe central or upper abdominal pain radiating straight to the back, nausea, vomiting, and a markedly raised serum amylase or lipase.
Gallstone Ileus Rare
A large gallstone (usually >2.5 cm) slowly erodes through the gallbladder wall into the adjacent bowel, travels through the intestine and impacts at its narrowest point — the terminal ileum — causing mechanical small bowel obstruction.
Accounts for fewer than 1–4% of all small bowel obstructions; more common in elderly women over 65. On X-ray the classic Rigler's triad — air in the bile ducts (pneumobilia), bowel obstruction pattern, and an ectopic calcified gallstone — clinches the diagnosis.
Advanced & Complex Gallbladder Conditions
These conditions require pre-operative planning, specialised surgical expertise, and sometimes a staged approach — they are not routine cholecystectomies.
Impacted Stones & Mirizzi's Syndrome
A stone deeply impacted at the gallbladder neck can externally compress the common bile duct — causing jaundice without a stone in the duct itself. Called Mirizzi's syndrome; classified into types by severity.
Gallstone Ileus
A large gallstone erodes through the gallbladder wall into the duodenum or colon (creating a fistula), then migrates into the small bowel causing intestinal obstruction. Rare but dramatic.
Cholecystoduodenal & Cholecystocolonic Fistula
Long-standing stone disease can erode an abnormal opening between the gallbladder and the duodenum or colon. Often discovered unexpectedly at operation.
Abandoned Procedures & Second Opinions
Some patients arrive after a previous operation that was stopped mid-procedure due to difficult anatomy, bleeding, or bile duct concern. Others seek a second opinion after being advised complex surgery elsewhere.
Gallstone Disease with Medical Comorbidities
Gallstones frequently coexist with diabetes, heart disease, thyroid disorders, and other systemic illness. Diabetic patients are at higher risk of severe cholecystitis. Patients on blood thinners need careful perioperative planning.
Special Situations
When gallstones travel beyond the gallbladder into the bile ducts or pancreas, management becomes more complex — each situation follows a specific treatment pathway.
Gallstones + Jaundice
CBD Stone / Choledocholithiasis
A stone that slips out of the gallbladder into the common bile duct (CBD) blocks the flow of bile — causing progressive yellowing of the skin and eyes, dark urine, pale stools, and itching.
Gallstones + Pancreatitis
Gallstone Pancreatitis
A stone temporarily blocks the ampulla — the shared opening of the bile duct and pancreatic duct — triggering acute inflammation of the pancreas. Presents with severe upper abdominal pain radiating to the back, vomiting, and raised amylase/lipase on blood tests.
Cholangitis
Bile Duct Infection — A Biliary Emergency
When bile duct stones cause obstruction AND bacteria get into the blocked system, cholangitis develops rapidly. Charcot's Triad: jaundice + fever + right upper abdominal pain. In severe cases it progresses to septic shock (Reynolds' Pentad: confusion + low blood pressure added).
Complex & Re-Do Cases
Previous Surgery / Mirizzi's / Fistulae
Some gallbladder conditions do not fit neatly into a standard pathway. These include Mirizzi's syndrome (stone compressing the bile duct), cholecystoenteric fistulae, and patients with a previous abandoned or incomplete operation.
Investigations & Diagnosis
The right investigation leads to the right treatment. Most gallbladder disease is diagnosed on a simple ultrasound. Bile duct problems and complications require more.

Ultrasound Abdomen
The primary investigation for all gallbladder disease. Safe, quick, no radiation. Detects stones (even tiny ones), sludge, polyps, gallbladder wall thickening, pericholecystic fluid, and a dilated bile duct. Most patients need nothing further.
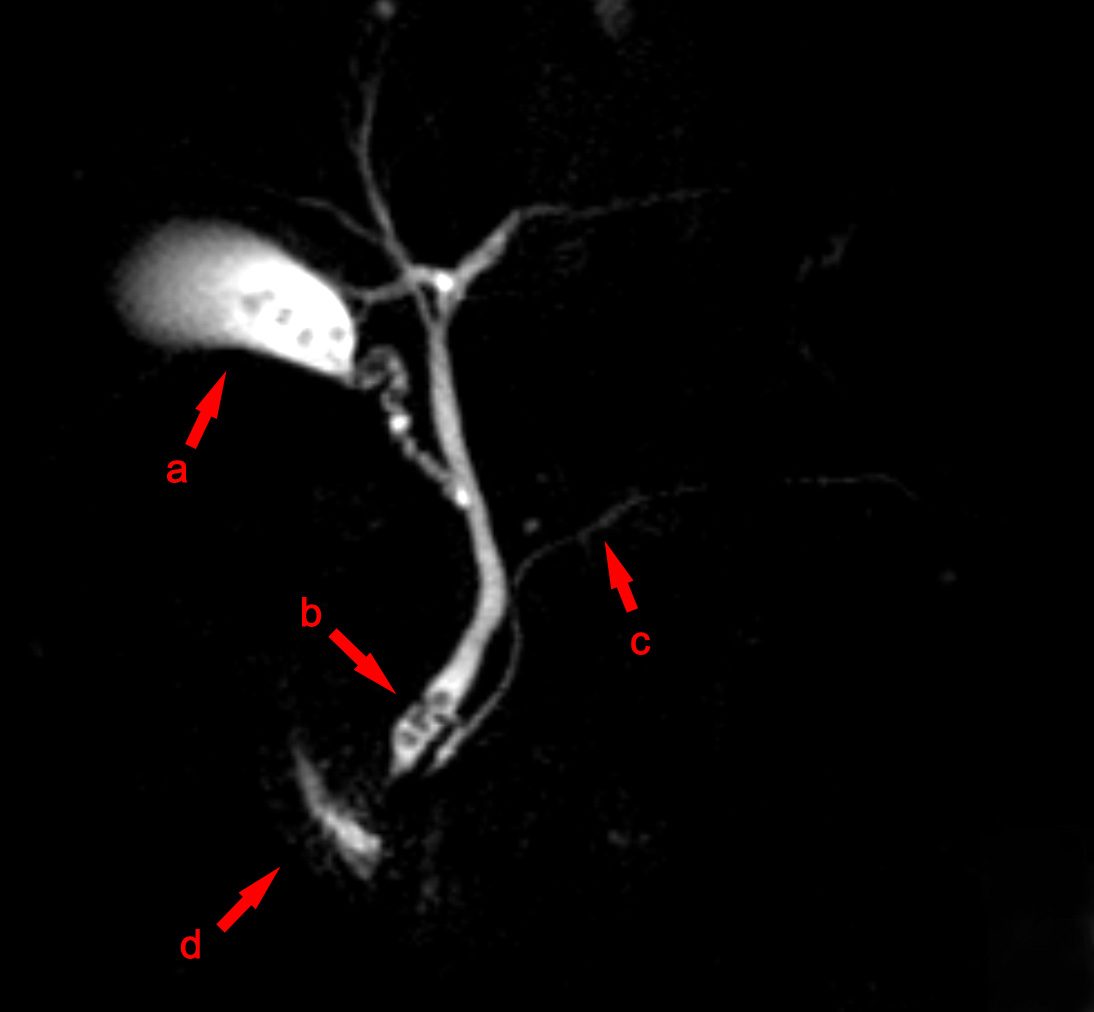
MRCP
Magnetic Resonance Cholangiopancreatography — a non-invasive MRI scan producing detailed road-maps of the bile ducts and pancreatic duct. Used when CBD stones, Mirizzi's syndrome, or complex bile duct anatomy is suspected. No radiation, no endoscope.

ERCP
Endoscopic Retrograde Cholangiopancreatography. Primarily a treatment procedure for CBD stones, jaundice, and cholangitis. An endoscope enters the bile duct opening; stones are removed and stents placed. Also provides precise duct imaging at the same sitting.

CT Abdomen
Used when complications are suspected — perforation, abscess, pancreatitis, or when surgery needs detailed anatomy. Not the first-line test for simple gallstones, but invaluable for emergency and complex cases. Blood tests (LFT, amylase, CBC) are essential companions to all imaging.
Management Pathways
Not every gallbladder condition goes straight to the operating theatre. The right treatment depends on the clinical situation, the patient's fitness, and the urgency.
| Condition | First Step | Definitive Treatment | Urgency |
|---|---|---|---|
| Silent gallstones | Observation / dietary advice | Elective laparoscopic or robotic cholecystectomy when indicated | Elective |
| Biliary colic / symptomatic stones | Pain management, low-fat diet | Elective laparoscopic or robotic cholecystectomy | Semi-urgent |
| Acute cholecystitis | IV antibiotics, IV fluids, analgesia, NBM | Laparoscopic cholecystectomy (within 72 hrs or interval) | Urgent |
| Empyema / pericholecystic abscess | IV antibiotics ± percutaneous drain (US-guided) | Interval cholecystectomy once infection controlled | Emergency |
| Perforated gallbladder | Emergency resuscitation, IV antibiotics | Emergency laparotomy / cholecystectomy with washout | Emergency |
| CBD stones / obstructive jaundice | ERCP — stone removal & stenting | Laparoscopic or robotic cholecystectomy (same admission) | Urgent–Elective |
| Cholangitis | Emergency antibiotics + ERCP within 24–48 hrs | Interval cholecystectomy after recovery | Emergency |
| Gallstone pancreatitis | Conservative (fluids, analgesia, NBM) ± ERCP | Early laparoscopic or robotic cholecystectomy before discharge | Urgent |
| High-risk patient with empyema | Percutaneous cholecystostomy under US guidance | Interval cholecystectomy when fit for surgery | Emergency–Bridge |
| Mirizzi's syndrome | MRCP workup, staging, sometimes ERCP stenting | Planned open or laparoscopic cholecystectomy with bile duct repair | Planned |
Percutaneous Cholecystostomy
For patients too unwell to tolerate surgery — those with severe heart or lung disease, the very elderly, or those in septic shock from empyema — a percutaneous cholecystostomy offers a safe, immediate solution.
Under ultrasound guidance, a thin drain tube is placed through the skin directly into the gallbladder. No general anaesthetic, no incision. Infected contents drain immediately — fever settles, pain resolves, and the patient stabilises. The tube remains in place for several weeks. Once the patient has sufficiently recovered, definitive cholecystectomy is planned.
In a small number of patients who remain permanently unfit for surgery, the cholecystostomy tube alone can provide long-term control — draining any recurring infection without an operation.
Surgical Treatment
Surgical Methods — Dr. Rajeev Kapoor
Three surgical approaches are used depending on clinical situation, anatomy, complexity, and patient preference. For most patients with uncomplicated disease, a minimally invasive approach — laparoscopic or robotic — offers the fastest recovery and best outcomes.
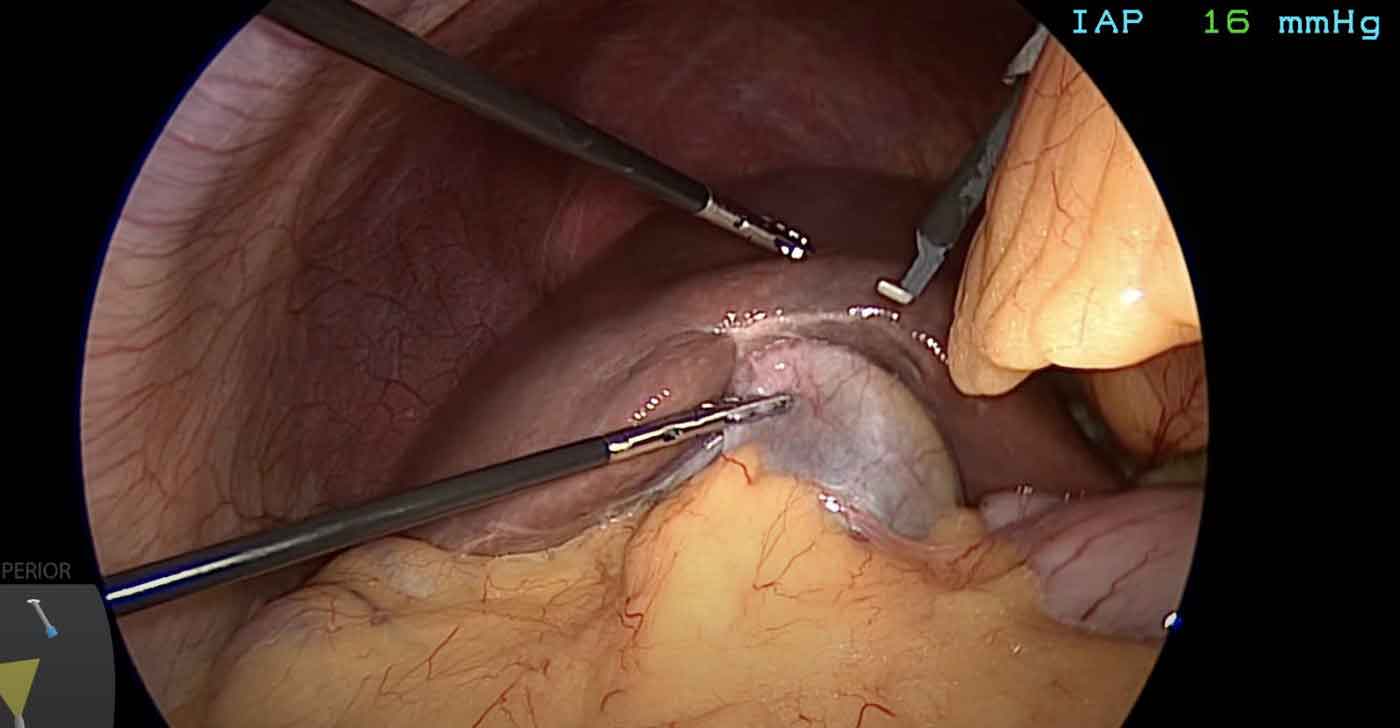
Laparoscopic Cholecystectomy
Performed through 3–4 small keyhole incisions (5–10 mm each) under general anaesthesia. A high-definition camera is introduced into the abdomen; fine instruments clip and divide the cystic duct and artery, then free the gallbladder from the liver bed. The gallbladder is extracted through one port.
Patients are typically discharged the same day or next morning. The tiny incisions cause minimal post-operative pain compared to open surgery, and recovery is dramatically faster.
- Day case or 1-night stay
- 3–4 incisions of 5–10 mm each
- Eating and drinking within hours
- Desk work in 1–2 weeks
- Full activity in 3–4 weeks
- Minimal visible scarring

Robotic Cholecystectomy — Da Vinci System
The Da Vinci robotic system is available at Fortis Hospital Mohali. The surgeon operates from a console, controlling wristed instruments with a magnified, high-definition 3D view of the operative field. Instruments have a far greater range of motion than conventional laparoscopy.
Robotic cholecystectomy is particularly considered in:
- Patients who specifically request it
- Mirizzi's syndrome (complex biliary anatomy)
- Dense adhesions from prior upper abdominal surgery
- Re-do or completion cholecystectomy
- Cases where tremor-free precision matters most
Insurance & Cost: Robotic cholecystectomy is covered fully or partially by a limited number of insurance companies. Many patients choose to pay privately. Coverage and costs are discussed clearly before your procedure. Your surgeon will advise whether robotic surgery offers a genuine clinical advantage for your specific case.
Open Cholecystectomy
A traditional open incision below the right ribcage — occasionally required when laparoscopic surgery is not safe. Situations include uncontrolled bleeding, anatomy that cannot be safely defined on camera, or extensive previous surgery preventing safe laparoscopic access.
Converting from laparoscopic to open when the situation demands it is sound surgical judgement — not a complication. Open cholecystectomy is also the primary approach in certain perforated gallbladder emergencies where speed and direct access are essential. Recovery is 5–7 days in hospital and 4–6 weeks at home.
Which Surgical Pathway Is Right for You?
Every patient's situation is different. This quick guide maps common clinical scenarios to the recommended surgical approach — your surgeon will confirm the right path for your case.
Day-care or 1-night admission. Keyhole surgery under general anaesthesia. Full recovery in 2–3 weeks.
Stones cleared from bile duct endoscopically. Gallbladder removed in same or next admission.
IV antibiotics, hospital admission, and surgery before discharge to prevent recurrence.
No delay. Laparotomy or laparoscopy with washout. ICU support may be required.
Pre-operative MRCP planning. Expert dissection. Staged or combined procedure as required.
Not sure which applies to you? Bring your ultrasound report and blood test results to your consultation. Your surgeon will map the right pathway within minutes of reviewing your case.
Your Journey from Symptom to Recovery
Understanding each step helps reduce anxiety and lets you prepare. Most patients move from first consultation to discharge within 2–3 days.
Preparing for Cholecystectomy
Getting to surgery safely involves a systematic pre-operative process. Here is what to expect from diagnosis to the day of the operation.
Confirming the Diagnosis
An ultrasound abdomen is the starting point for most patients. If bile duct involvement is suspected, MRCP is arranged. Blood tests — liver function, full blood count, kidney function, blood sugar, and clotting — are ordered. All imaging and reports are reviewed together before any decision is made.
Pre-Anaesthesia Check (PAC)
A formal assessment by the anaesthesia team. This includes a review of your full medical history, current medications, allergies, previous anaesthesia reactions, and fitness for surgery. An ECG and chest X-ray are ordered for patients over 40 or those with heart or lung conditions. Any issues are optimised before the operation date is fixed.
Medication Review
Blood thinners (warfarin, aspirin, clopidogrel) are typically paused before surgery — usually 5–7 days beforehand, in liaison with your cardiologist or physician. Diabetic medications may need adjustment around the fasting period. Never stop any medication without your surgeon's specific guidance.
Consent & Discussion
The operation, its alternatives, specific risks (bile duct injury, bleeding, conversion to open, anaesthetic risks), and expected recovery are explained clearly. You have full opportunity to ask questions. Consent is documented formally — nothing is rushed.
Fasting & Admission
You will be asked to fast for 6 hours (solid food) and 2 hours (clear liquids) before your operation time. Most laparoscopic cholecystectomies are planned as day-surgery or one-night-stay procedures. Bring a list of your medications and any recent blood reports on the day.
What to Expect on the Day
You are received in the ward, seen by the surgical and anaesthesia team, and shifted to the operating theatre when ready. The operation typically lasts 30–60 minutes. You wake up in the recovery room, then move to the ward. Most patients are walking within a few hours and eating a light meal by evening.
After Surgery — Questions & Answers
The questions patients ask most in the days and weeks after gallbladder surgery.
Who Is at Risk?
Gallstones do not strike randomly. Certain factors — many of them highly prevalent in the Indian population — significantly raise the likelihood of stone formation.
Female Sex
Women are three times more likely to develop gallstones than men. Indian data confirms: 5.59% prevalence in women vs. 1.99% in men. Oestrogen increases cholesterol secretion into bile; progesterone slows gallbladder emptying.
3× higher risk in womenPregnancy & Multiparity
Each pregnancy elevates oestrogen and progesterone, both of which promote stone formation. The gallbladder empties less efficiently during pregnancy, allowing bile to stagnate and crystallise. Risk rises with each successive pregnancy.
Hormonal Contraceptives & HRT
Oral contraceptive pills and hormone replacement therapy both raise oestrogen levels, increasing cholesterol concentration in bile and reducing gallbladder motility.
North Indian Diet
High intake of ghee, refined carbohydrates, saturated fat, and low dietary fibre — common in North Indian diets — promotes cholesterol supersaturation of bile. North Indians have 2–4× higher gallstone prevalence than South Indians.
2–4× higher in North IndiaDiabetes
Diabetes significantly impairs gallbladder motility, causing bile stasis and stone formation. Indian studies show diabetic patients have a 4.27× increased risk — particularly relevant given India's 101 million diabetics.
4.27× increased riskFamily History
A striking 69% of Indian gallstone patients report a positive family history. Genetic factors influence bile composition, gallbladder motility, and cholesterol metabolism — all of which contribute to stone formation.
69% have a family historyObesity & Rapid Weight Loss
Obesity increases cholesterol secretion into bile. Paradoxically, crash dieting or rapid weight loss (common in urban India) is equally dangerous — the gallbladder sits idle during fasting, allowing bile to concentrate and stones to form.
Age
Risk rises progressively after 40. In India, most symptomatic gallstone patients present between 40 and 60 years of age. Bile composition changes with age, and gallbladder contractility gradually declines.
Can Gallstones Be Prevented?
Not all gallstones are preventable — genetics and hormones play a role beyond our control. But lifestyle choices significantly influence your risk, and small consistent changes make a real difference.
Eat at Regular Times
Skipping meals allows bile to sit concentrated in the gallbladder for hours. Three regular meals — including breakfast — keep bile moving and reduce stasis.
Increase Dietary Fibre
Fruits, vegetables, whole grains, and legumes reduce bile cholesterol and speed intestinal transit. Replace refined carbohydrates and white rice with whole grains where possible.
Moderate Ghee & Saturated Fat
Ghee is not the enemy in small quantities, but daily high-volume use raises cholesterol in bile. Cook with less ghee; use plant-based oils for everyday cooking.
Stay Well Hydrated
Adequate fluid intake keeps bile dilute and less likely to crystallise. Aim for 8–10 glasses of water daily — more in summer or with physical work.
Maintain a Healthy Weight
Lose weight gradually — no more than 0.5–1 kg per week. Rapid weight loss sharply increases stone risk. Regular physical activity improves gallbladder motility directly.
Control Your Diabetes
Good glycaemic control reduces the gallbladder stasis associated with diabetes. If you are diabetic, a baseline abdominal ultrasound is worth discussing with your doctor.
Already have gallstones? These measures will not dissolve existing stones, but they reduce the risk of new ones forming after surgery and support your overall digestive health.