


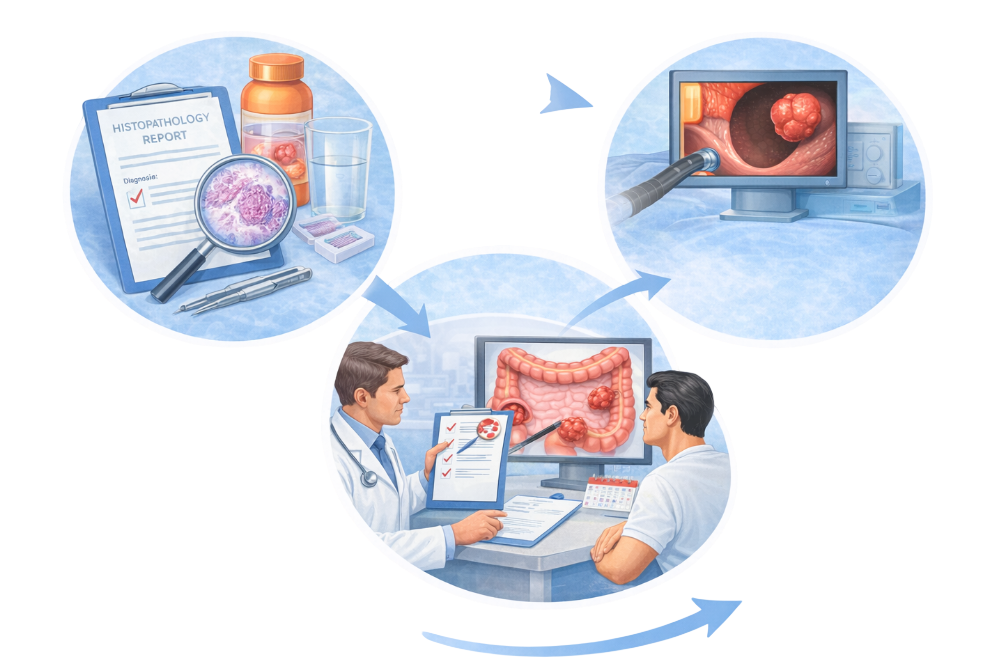


When do I Need a Colonoscopy
What is Colonoscopy? A colonoscopy is a test utilized to find lesions or irregularities in...

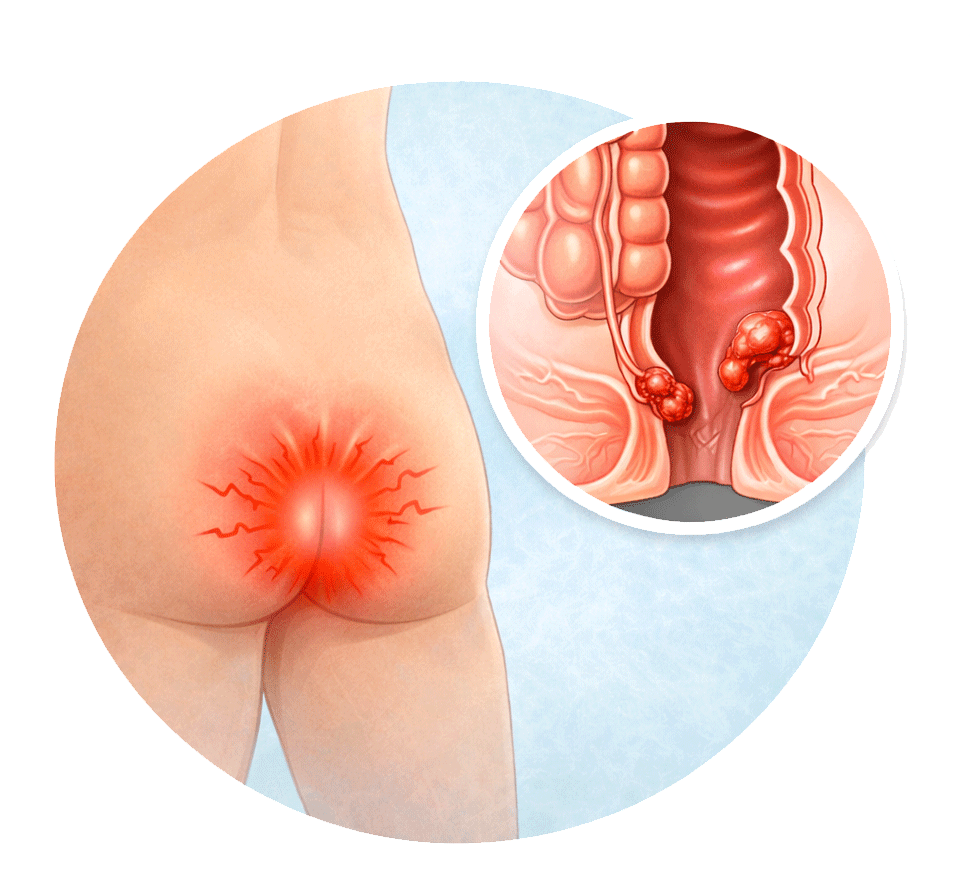
What is sphincter preservation surgery for Rectal Cancer?
Surgeons frequently remove both the rectum and the anus from patients who have colorectal cancer...
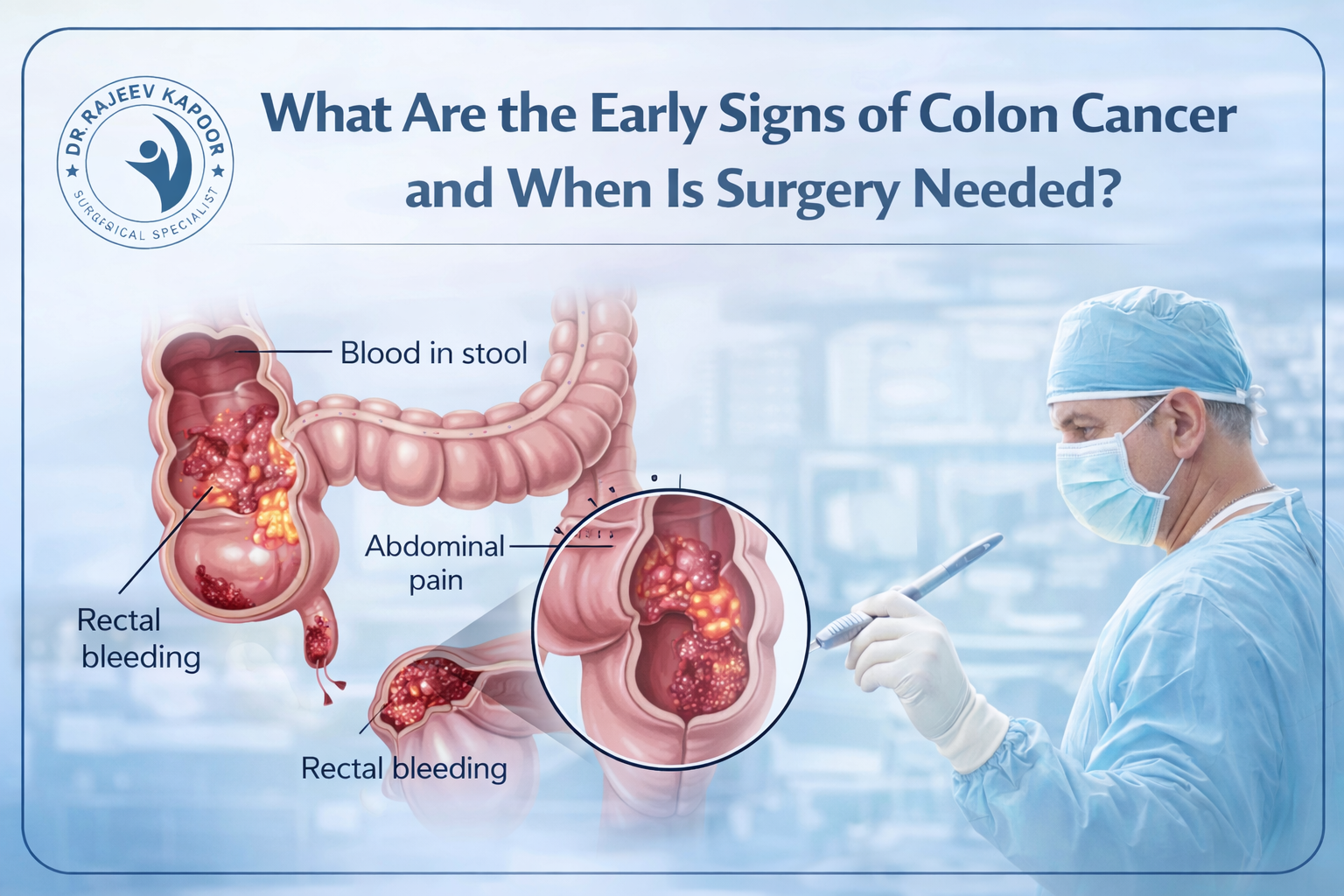
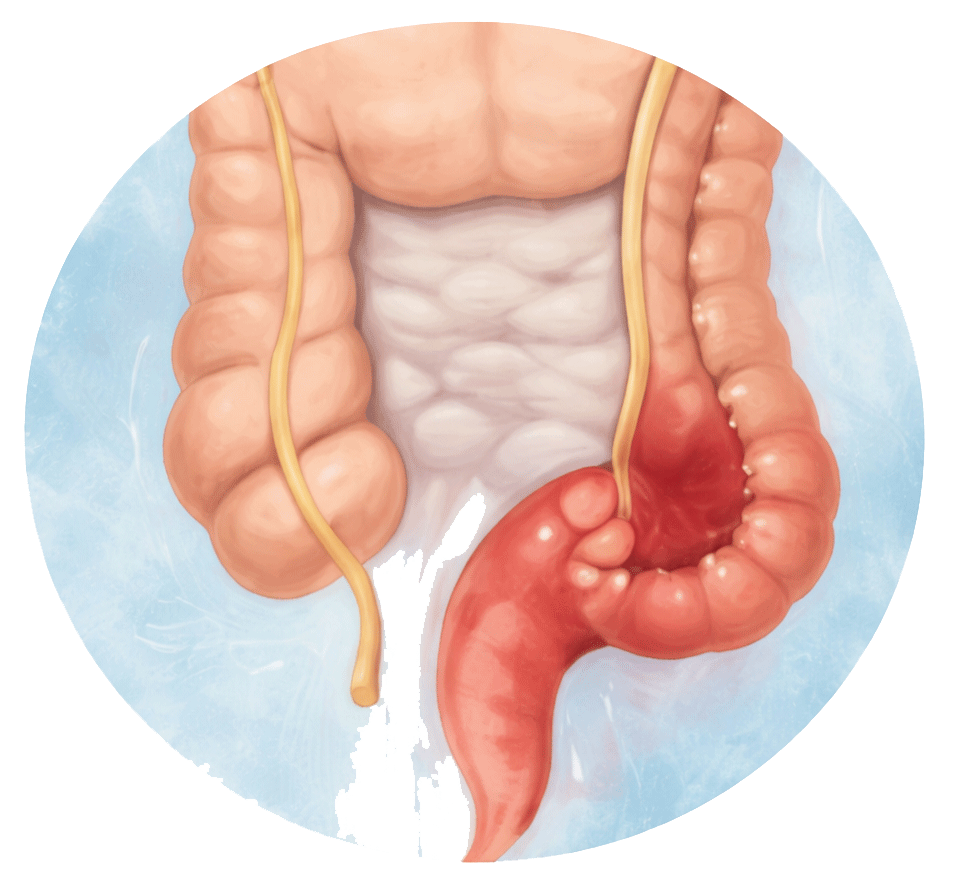
What Are the Early Signs of Colon Cancer and When Is Surgery Needed?
Colon cancer is one of the most common gastrointestinal cancers worldwide, and its incidence in...

Vulvar Cancer Treatment Doctor in Chandigarh | Vulvar Cancer Surgeon
What is vulvar cancer? Best Treatment for Vulvar Cancer – Vulvar cancer can happen on...

Understanding Right Colon Cancer: Symptoms, Diagnosis, and Treatment Options
Understanding Right Colon Cancer: Symptoms, Diagnosis, and Treatment Options Right colon cancer, also known as...
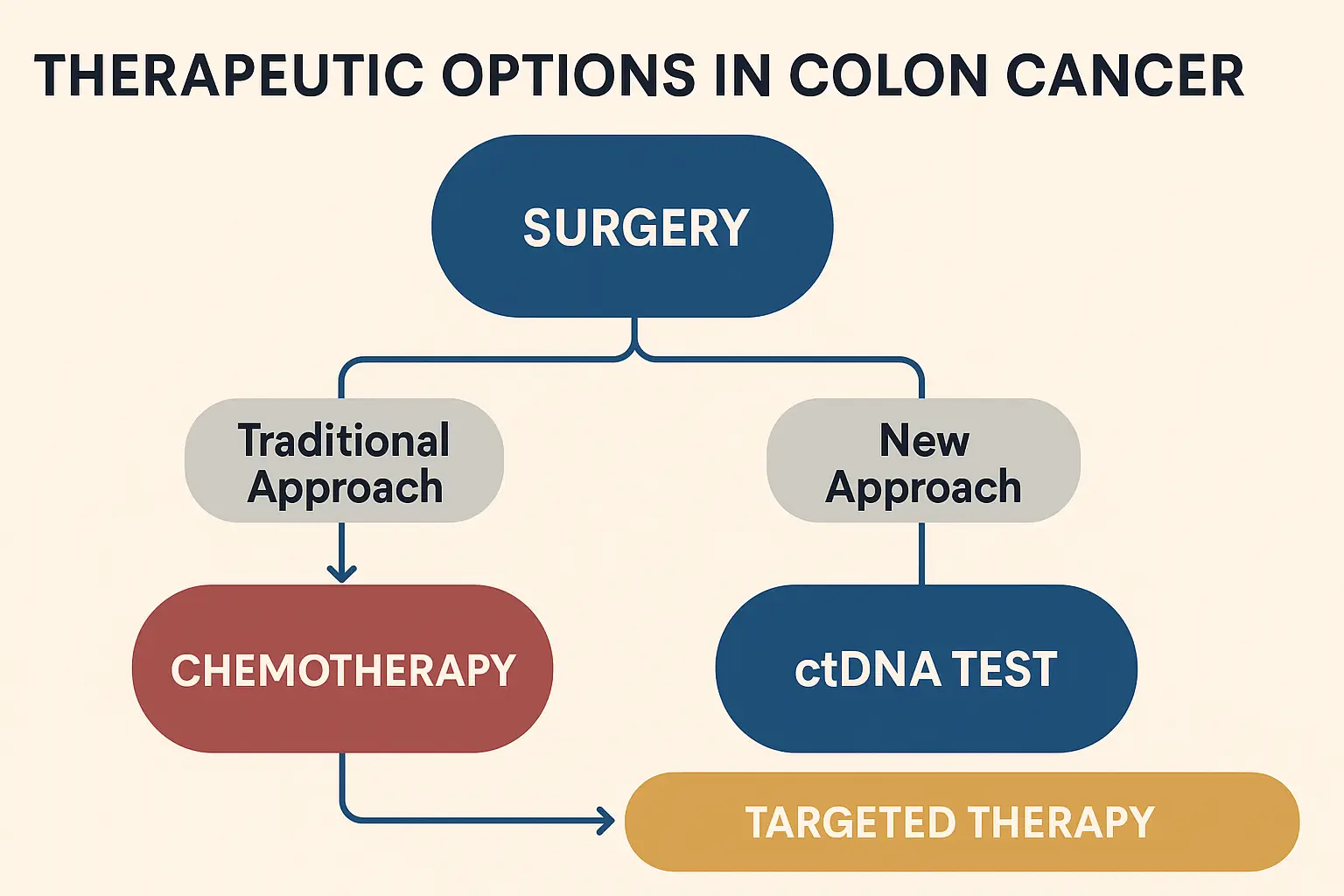
Therapeutic Frontiers in Colon Cancer: What’s New in 2025
Treatment for colon cancer (colorectal cancer) is undergoing a major transformation. Once dominated by surgery...